|
It was 2015 and I was just getting started with my new practice. A breath of fresh air. After years of working inside the health system, I realized the focus is managing illness, not wellness. The focus was not on building relationships with your patients, getting to know them beyond the small talk, learning their story, meeting those who care for them, and definitely not on making health care delivery simple and efficient. I had no idea where this career move would go. I was nervous and scared of course, but happy.
I was rounding at the hospital as a hospitalist as I was still building my new practice when I met a wonderful young man. On my patient list it had said pneumonia as the reason for his hospital stay. I entered the room in my usual way, a knock, a wave, as I walked in with a big smile. “Hi there! I’m Dr Ahmed, just one of the hospital medicine doctors. How are you?” I said, not realizing my world was about to change. He managed to smile despite how ill he was from this long hospitalization. His family was at the bedside and greeted me upon entry. As this was my first time meeting him, I summarized his care so far to demonstrate to the family and him that I reviewed his chart in detail before coming so they can rest assured I will smoothly take over his care from my partner. He had an immune disease that made him susceptible to recurrent pneumonia. Each time he had pneumonia, the bacteria became more resistant to the antibiotics used to treat him that we literally came down to 1 antibiotic that would kill this bug. In addition, his lungs were getting scarred with each illness, leaving less viable lung tissue that could provide him oxygen. His family started to share his story. They shared with me how he has been battling not only his multiple pneumonias, but also his insurance company. They were taking him to multiple appointments between pulmonologists, infectious disease, immunologists, and multiple tests. The patient and his family could tell when a pneumonia was developing but by the time they would get a hold of the right doctor, he was already in trouble. He would be rushed to the ER. This routine was not only exhausting but kept putting him in the hospital. I listened to them carefully. By this time I had found a comfortable spot on the windowsill to sit. My brain was flooding with emotions. I was frustrated by the thought of this young man getting hospitalized multiple times and being away from family and friends. I was upset with the system that was not communicating properly and how difficult it was to get a hold of someone to get him the care he needed. If the family can tell when a pneumonia was starting, why was it so hard for them to get the treatment they needed to prevent a hospitalization? Then I was amazed. This young man still smiles and says “thank you” and “please” and “sorry to be a pest, but…” If I was in his shoes I probably would be upset and angry all the time! Not him. That was not in his DNA. He was different. He was unique. He was kind at heart. I slid off the windowsill as my mental clock screamed “Time is up! You need to see the rest of your patients! Hustle!” I fought this thought away and re-focused. You see, when you work in the system, we all have a mental clock that keeps us moving. Ten minutes here, five minutes there, this is how we get through rounds at a reasonable time with an average patient list of 15-18 patients all with multiple health issues happening at the same time. But, this time, I was different. I was not working for the system anymore so I was in charge of my time, not the system. I shared my practice with them and my frustration with the system. I told his family they are our teammates in caring for him. Therefore, all necessary resources must be readily available to them when they identify a health crisis is at hand. There should be no phone trees, voicemails, instead a human being there to help. That was my vision for health care. So I took him on as a patient in my private practice. I left the room with hope and determination to change the patient experience. In the following months and years, we battled his health insurance to cover an antibiotic that was the only one that would kill the bug causing his pneumonia. Several appeal letters were sent and we received denial after denial. His family, by the Grace of God, had a resource in the family who was able to get samples of this antibiotic. So, we hoarded this medication to treat him. It is absolutely amazing how the most powerful nation in the world allows its citizens to have to experience this much difficulty in seeking medical treatment. He went to Mayo in Minnesota and my team and I directly discussed his case with the team there. The Mayo team appreciated the communication and were able to treat him. He also was evaluated for a lung transplant. Initially he was denied and was high risk. We went to Texas for another opinion and they agreed to give him a chance with a lung transplant! I have to pause and share with readers how significant this is. I did a video call and he was in his apartment prior to transplant. He took multiple medications and nebulizer treatments just to keep breathing. His entire day was involved in helping his lungs oxygenate. Despite all of these challenges, he kept working at his job. He was determined not to miss work. Even when he was at the hospital, he would try to get work done. How incredible is that?? You have to understand, work gave him a purpose to fight and he deeply cared for his customers. He cared about his employer and his team. He embraced his responsibility. Throughout his illness, I was so amazed at how flexible his employer was with him. It seemed like the entire company were his cheerleaders and they were ready to help him along the way. It is a tremendous lesson for all employers. While I took care of his health issues, he was teaching me about resilience, kindness, the importance of having a positive mindset; and showing me how to treat my future employees and how important an organizational culture of compassion would be for my future team. It truly was a privilege and a blessing to have this incredible experience. After his lung transplant, he had about 2 years of incredible health. He was breathing better, having full conversations without coughing, walking without oxygen, and just doing great. My subsequent visit with him was incredible. Here is someone who would be constantly coughing throughout the conversation and now his voice was strong. Over the next few months, we started to develop a pneumonia here, a cough there, and he was treated accordingly. But, soon, on CT imaging, we started to see what we all feared. The scarring of his lungs started. It truly was a “oh shit” moment as I reviewed his images one day. Despite this, he battled with a smile and kindness. As a physician, there are times when you look at a radiographic image or set of lab results where you have a gut wrenching thought. While you wrestle this horrible thought, you become mindful of the surrounding glare from the patient and their family members. You have to quickly be mindful that although you have a bad feeling about something, you must reserve that thought until you complete the work up. Every physician has that feeling, that concern or belief, when they first see chaos on paper or radiographic image. At the same time, you must keep your composure and prepare the patient and their family members for what may lay ahead. After several more months, while I was rounding at the hospital, I received the dreaded phone call. As I was whooshing room to room like a downhill skier maneuvering the halls and going room to room, I stopped and stared at my phone. “LiveActive Member” it read. Before I answered the phone, I had a terrible feeling it was him. It was. He had called because he was having excruciating pleuritic chest pain. This was pain each time he took a breath. As his lungs expanded, the nerve fibers burned with pain signals bursting at the seams. He had this before and we were able to calm it down with medications, but this was different. He was screaming in pain and could not even complete his sentences. I calmed him down and knew this was a losing battle. We ultimately had to send him to the hospital. His oxygen needs increased while the team worked on his pain. He started to require very high concentration of oxygen. Even then, he was insistent on getting home so he can return to work. But his body would not comply. His lungs continued to fail and he agreed to hospice care while in the ICU. I finished up my last patient at the office and made the final click of my mouse to close all the windows on both computer monitors. I closed my eyes. It was an exhausting day. My wife, our Chief Operating Officer, came to my office. The two of us are the last to leave the office for many years. We both enjoy the quiet after hours that fill our office after our entire team heads home after a hard days work. "You should go visit him tonight," she said with a soft voice after she had settled quietly into one of the chairs across my desk. I was still staring at my black monitor screens, just exhausted from the day. My feet felt heavy. "I can drive and you just sit and relax. Or I can just go with you to keep you company!" She said in her usual upbeat excited voice. The two of us headed out, left her car in the parking lot, and got in my car to head to the hospital. Once we arrived to the ICU, I met his family and shared my condolences. I then walked over and held his hand. I was relieved. He was finally comfortable. He wasn't struggling to breath, he wasn't in pain. He was truly resting. He was on some sedative medications and on high flow oxygen. His family shared with me that they were trying to get him on lower oxygen to move him to the hospice floor and he was now full comfort care. While we visited, we shared stories, had some laughs as we reflected on some stories, and reflected on all the challenges we all went through while taking care of him. I turned towards him as I was saying goodbye to the family and noticed his chest rise was getting more spaced out. Something in my gut was telling me his time is very near. It was as if he was listening to our stories, our laughs, and when I stood up to leave, his soul was content and ready to move on. It was an incredible experience for me. As I said a final prayer for him, I left the room. My phone buzzed at 2 am. "LiveActive Member". It was his mother texting me that he had passed. You would think that I would burn out by allowing myself to be so close to my patients? It is actually the opposite. Prior to starting my private practice where I create real relationships with my patients, I was just working shifts. Getting through the day. When I did experience a patient death, it was usually anger. Why did the system not allow them to get their meds that may have caused this stroke or heart attack or preventing appropriate follow up, etc? Now, I have the privilege to battle with my patients. Fight for them, think with them, guide them as they navigate our health care maze. You feel you gave it your all and patients and their families take notice. You do it together. You battle together. What an honor and privilege to be part of such a significant aspect of human life. Why do physicians give up this incredible opportunity? How have we allowed the business of health care to become more like the manufacturing industry - volume over quality. And if quality is being incentivized, it is surrounded by heavy regulations where the cost of achieving quality service is greater than the reimbursement. So why do it? Our health care system is on the verge of massive change. Many physicians have already taken back control of their profession and career by going back to private practice. Ultimately, the support of our patients is what helps us achieve this goal. Your support, allows us physicians to think more clearly, give our patients a little more, strengthen our family bonds who support us and help us be most effective on a daily basis. As many thank you's I get from my patients family members, I tell them "No, thank you for supporting me to do this." - Dr Ahmed
0 Comments
Remember the days when commercials of men and women swimming up to the screen with big smiles would shake their luscious wet hair to show off how an expensive hair product helped them grow their hair? These were expensive treatments that required continuous treatment and the minute you stopped using the product, hair loss would return. This happens because the treatment is temporary. Fast forward to today and we now have a treatment option that uses YOUR OWN GROWTH FACTORS to stimulate hair growth. Studies have shown platelet-rich plasma (PRP) stimulates hair growth naturally. Current treatments include Minoxidil, which comes in pill form or foam shampoo. There are different concentrations of Minoxidil, but 5% has shown to be most effective. The pill form of Minoxidil comes with potential side effects, which includes cardiac side effects. Other treatments include Finasteride. This is a oral pill that is taken daily and again, has potential side effects. Finasteride is not FDA approved for use in women and actually is a category X medication, which means it cannot be used in pregnant women. So, it becomes obvious PRP is the way to go. In addition, studies have shown microneedling after PRP injection improves hair growth. Here is what the PRP process looks like: 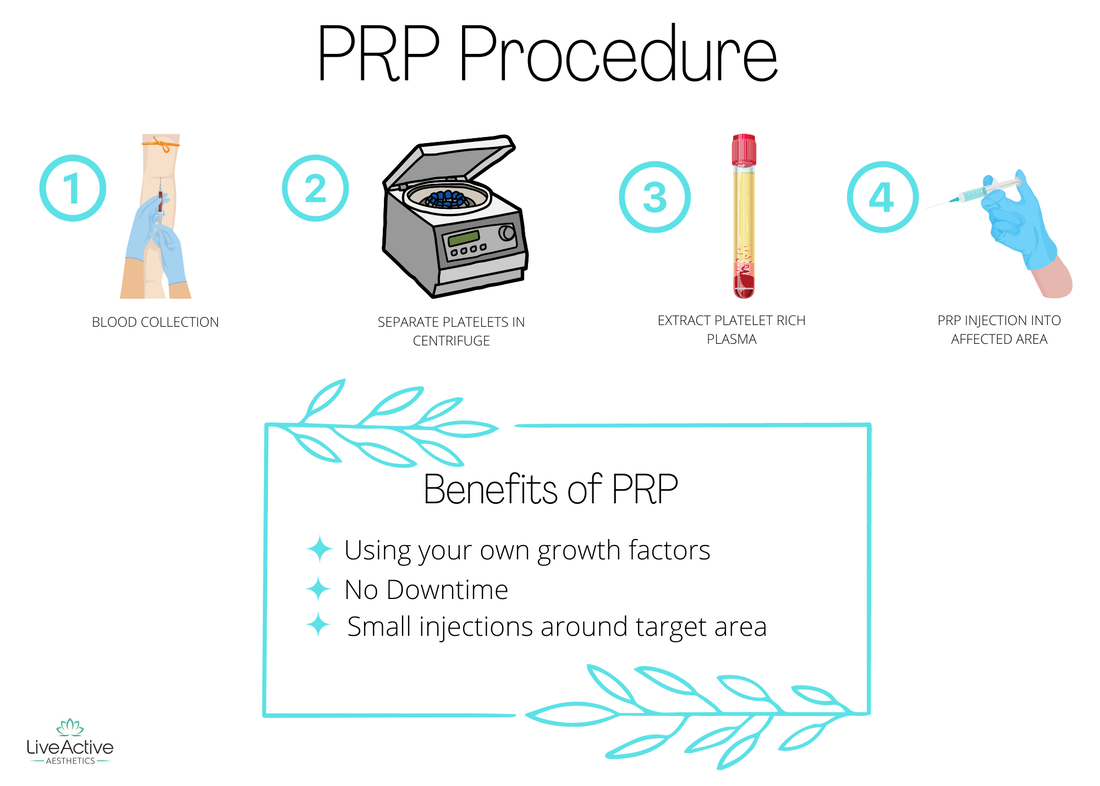 www.LiveActiveAesthetics.com for more information Here is a quick look at the anatomy of a hair follice: 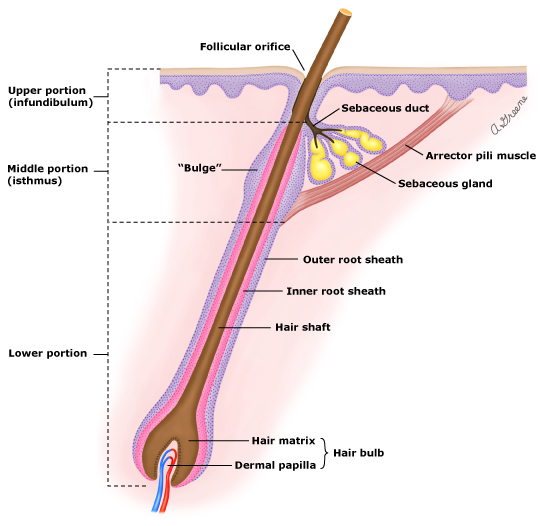 * We inject at the "Inner root sheath" or just above the "hair bulb". So exactly, which growth factors are in PRP? Here is a list:
Studies have shown that people have the most benefit with 4 treatments which can be spaced as early as weekly or the preferred monthly treatments. Some may choose not to numb the scalp, but I prefer to keep the patient as comfortable as possible. My team and I numb the area to assure our patients are as comfortable as possible. Since these growth factors are your own, there is no rejection or allergic reaction. This is a natural way of facilitating hair growth. PRP can also be used with facial microneedling procedures with SkinPen. This helps with eliminating scarring, acne, wrinkles, and tightens the skin. There are many innovations taking place in the practice of medicine and LiveActive intends to bring these innovations to our patients at an affordable price. I hope this blog of educational and informative. As fall begins, this is the time to consider laser treatments like BBL, Halo, PRP, and microneedling. This is all part of living healthy and maintaining our largest organ of our body - OUR SKIN! Dr Ahmed  Unfortunately, as with any piece of health news, there are lots of social media posts, articles, and opinions. The purpose here is to set the record straight and hopefully be concise and informative for my readers. So here it goes:
WHAT THE HECK IS "MONKEYPOX"? No, it does not come from monkeys and the planet of the apes will not become a reality. Stop it. Monkeypox is a viral zoonotic infection that results in a rash similar to smallpox. It is an orthopoxvirus that is in the same genus as variola (causative agent of smallpox) and vaccinia viruses (virus used in smallpox vaccine). TELL ME A LITTLE MORE ABOUT THIS LITTLE GUY... Monkeypox was first isolated in Denmark in the late 1950s from a colony of monkeys from Singapore that were going to be used for polio virus research. In the decades that followed, there were more outbreaks in lab animals in the US. The first disease in humans was identified in 1970s in the Democratic Republic of the Congo. Since the discontinuation of smallpox immunization, which does protect against monkeypox, most cases have occurred in Central and West Africa. In the US, the first cases were seen in 2003. Since that time, there were a few cases popping up here and there which were mostly due to travel. SO...WHAT IS ALL THE EXCITEMENT ABOUT? Between 2018 and 2021, 7 cases were diagnosed in the United Kingdom. 4 of these cases were related to travel to endemic countries and 2 cases resulted from household transmission from one of the travelers and 1 health care worker acquired it through contact. Fast forward to 2022. Let’s go to Europe where we see the reported case. By July 2023 World Health Organization (WHO) declared a public health emergency of international concern. Thousands of confirmed cases in dozens of countries were reported. HOW DO WE GET INFECTED?
Once lesions are scabbed over and new tissue is being produced, the infectivity risk is reduced. WHAT ARE THE SIGNS OF ACUTE INFECTION? Every bug likes to “cook” for a bit in the human body – otherwise known as incubation period. This is the time period from exposure to onset of symptoms. Monkeypox ranges from 5-13 days but can also range 4-21 days.
WHO IS AT MOST RISK FOR INFECTION AND POOR PROGNOSIS?**Immunocompromised individuals. These include anyone with history of active cancer, on active chemotherapy, taking medications that suppress their immune system. RISK OF DEATH? Very low, especially in the US. Hospitalizations occurred due to pain control, secondary infections, and had favorable outcomes. WHEN SHOULD AN INFECTION BE SUSPECTED? Rash WITH other symptoms AND exposure history. Since this virus is transmitted through close human contact with respiratory secretions, any genital lesions with exposure history must be investigated. WHAT LAB TESTS SHOULD BE ORDERED? Viral testing – Polymerase chain reaction (PCR) test. Skin lesions or abscesses can be cultured as well. Throat swabs are available but not used to confirm diagnosis. HOW CAN WE PREVENT THIS? Isolation and standard precautions. PPE use in health care settings helps spread of the virus in the hospital.
ANY TREATMENT OPTIONS? No Ivermectin please. Tecovirimat is the first antiviral indicated for the treatment of smallpox that was approved in 2018. Brincidofovir, analog of cidofovir, was approved in US 2021. Both of these agents are not available for commercial sale. Vaccination for smallpox eradicated this from the world. Now with growing cases of Monkeypox, vaccinations are starting again. But again, these are not readily available at this time. US has 2 vaccines in its stockpiles: JYNNEOS and ACAM2000. CDC does not recommend widespread vaccination against monkeypox at this time Here is a list of phone numbers for KS health departments:
Currently, no widespread vaccination programs in MO and KS, but both states have stored vaccines. Please review CDC website for more information. Cheers, Dr Ahmed  Human beings are not meant to be static beings. The human body is dynamic. It does an incredible job at adapting, cleansing, healing, and building to treat and prevent injury. It does all of this instantly. The human body recognizes challenges, adjusts its processes and mechanisms to address and resolve those challenges. It is absolutely incredible!
Therefore, change is a natural phenomenon for all of us. So why is it so hard for us to make changes? Why do we fall short of our goals? Why do we say things like "I wish I could..." or "If only this didn't happen, then I would have done..." Each one of us can achieve great things. Whatever dreams we have, we can achieve. The solution is our mindset, our life philosophy. Here are 3 key elements to making dramatic life changes. 1. Understand that we ALL have similar experiences, but the difference is how we respond to it. "The same wind blows on us all; the wind of disaster, opportunity, and change. Therefore, it is not the blowing of the wind, but the setting of the sails that determine our direction in life." - Jim Rohn We must learn from the experiences that happen to us. Those who have faith may recall ancient stories where God says He puts us through experiences to teach us, to prepare us, so that we are ready to achieve our dreams. We may think we are ready, but we're not. Experiences may happen to us so that we learn certain lessons like what can go wrong, what elements or structure needs to be in place, and what kind of people we may need to surround ourselves with in order to achieve our goal. There is always a Master Plan and our job is to navigate, learn, adapt, and keep moving forward with gratitude. Knowledge and experience make us stronger, informed, and more prepared. I am telling you, majority of the time when we embrace this mindset, our success will be far greater than the goal we had originally set for ourselves. 2. There are certain things that will not change. Seasons and time won't change. Similarly, bear markets and bull markets will come and go. Interest rates will fluctuate. Taxes will exist. All these things will not change. Once you understand this, your mindset completely changes. In the economic summer, you will prepare for winter. In a bull market, you will prepare for a bear market. When interest rates are low, you prepare for rates to rise. Once you achieve this mindset, you perceive challenges with ease. No challenge is ever too great to conquer. You embrace and appreciate each moment as every experience in life has a purpose and value. 3. You must be willing to change "Don't wish it was easier, wish you were better. Don't wish for less problems, wish for more skills. Don't wish for less challenge, wish for more wisdom." -Jim Rohn What drives you? What do you enjoy? Figure out what gets you excited about life. Once you figure out what gets you going and what hinders your progress, then your mind and body will be fueled with energy. Maybe you need to get away from negativity, stop watching the news, mute certain text messages, leave certain social media platforms to allow yourself to immerse into what you enjoy. Get moving physically and emotionally. Learn how to make yourself better, how to apply what you learned to your daily routine. Stop being a drifter in life and take an active role. Look forward to each week, each day, each hour with certain goals. Imagine what you can accomplish in a month, a year, a lifetime with this discipline! Finally, write things down. Hold yourself accountable. If you are trying to lose weight, then the formula is burn more energy than you consume. Use MyFitnessPal and other apps to document your meals, create a excel spreadsheet to document your workouts, have a plan. Each day, reflect on your progress and make short term goals that work towards your ultimate goal. These 3 principles will bring dramatic change into your life. Focus on implementing them today so that change will come as soon as tomorrow. To a life filled with gratitude, Dr Ahmed It was one of those hot and dry summer days in Kansas City. It was about mid-day. I adjusted my necktie and walked into our small humble conference room in my newly built Direct Primary Care office to meet a potential new member. This was a “meet and greet”. I was a young physician who just started on a new journey to bring change to our health care system.
You see, I had been an employed hospital medicine physician for 5 years prior to this moment and I had come to realize that primary care was in dire need for a real make over. It is the foundation of our health care, the gatekeeper, the seed that if planted just right and is cared for, it can blossom into something special with good health outcomes. I had seen enough. I had set out to eliminate financial barriers, system barriers, and communication barriers that were in the way of providing good primary care services. The current health care system rewards “sick” and “reactive” care. When the truth is that primary care can handle 80-90% of your health care needs and PREVENT downstream costs and illnesses. We need to flip the current paradigm of specialists first with primary care for cough and colds, to PRIMARY CARE, THEN specialists if they are needed. And if they are needed, let's get their help and then have them leave the party. Crowded parties are messy, loud, confusing, and we can barely hear each other talk! As I entered the conference room, I was met by a sweet young woman who was dressed in a full sleeve shirt and jeans on this scorching summer day. I was immediately intrigued and curious. I smiled and greeted her as I usually do with these “meet and greet” meetings. After a few pleasantries and small talk, she said, “I heard about your practice from my nutritionist after I was complaining about how I feel like a pinball in our health care system. No one is giving me answers to my questions.” I nodded my head. Many people in sales and other professions can relate to how her statement initiated a response in my head instantly. All the things you say and the stories you share in your marketing strategy come forward in your brain itching to spill out of your mouth. My brain was screaming, “I know! I have heard this a million times! This is why I am here!” But, I stayed calm and nodded. She then went on to roll back her sleeves. It felt like it was in slow motion, because the rash that was living underneath that shirt was so red and angry that although my eyes widened, I made sure my mouth stayed closed. I was speechless. This rash went up to her neck and she told me it even covered her legs and back. It was remarkable. I assured her I would give her the best care I can and review the work up she had completed. After a little more questioning and back and forth, she was satisfied and signed up for our services. Over the next few weeks, I was able to review her case in detail. It turns out, she had a skin biopsy done, but somehow there was no action taken based on that biopsy because the conversation stopped. She did not have health insurance. The treatment would cost too much so everything halted at that moment. I presented this case and the biopsy results to another dermatologist using a Telemedicine service that is FREE for our patients to see if the treatment I was considering for her would be reasonable. The medication I wanted to use was much more affordable cash price and I could dispense it at our office for her. The dermatologist agreed and we started the treatment. After a few weeks on the treatment, her RASH DISAPPEARED! She wore short sleeve shirts again and flip flops. She was ecstatic. Primary Care wins! After about a year or so, she had a cough that would not go away. She was feeling ill and short of breath. She continued to smoke cigarettes, so we ordered a chest x-ray to look. She had been treated with the usual steroids and inhalers with the occasional antibiotic. The x-ray showed a spot that was concerning. The cost of the xray was $35. Knowing she did not have health insurance, I discussed with her about getting a CT scan of her chest. This would be around $300 cash price. We decided to move forward with it and get the CT scan. Within the next day she had her CT scan and by this time, she was more breathless. I reviewed her CT scan and sat back in my chair a second time...speechless. There were lesions that looked concerning for cancer everywhere in her lungs. Lymph nodes were also enlarged, suggesting possible spread of the cancer. So, here you have someone who has no health insurance and facing something that may potentially harm her and make her bankrupt in a matter of days. I called the Oncologist and Pulmonologist at the hospital. I then called the case manager at the hospital to review the case and see if we can get her qualified for Medicaid. Then, I called the ER physician to explain our master plan. We needed to admit her to the hospital to get all the necessary imaging completed and a biopsy, while we get her breathing better. However, we also wanted to assure she would qualify for Medicaid given our concern for cancer. It is with this game plan I finally called Cindy and said, we have to go to the ER and my team is ready to give you the best care possible. Later, that evening, I drove to the hospital after I finished seeing my patients at the office. By this time, the Oncologist and the Pulmonologist had met with her, CT of her Abdomen and Pelvis were completed, breathings treatments had started, and other treatments were occurring at the same time. Her ER room was full of family members. I could feel each of their eyes fixated on me as I passed through the curtains to enter her room. I was greeted by her smile that even surpassed the oxygen mask she had on. She was feeling better already. I answered multiple questions from her family and laid out a potential hospital course that would soon follow. After a few days, she was discharged from the hospital and started the merry go round of seeing specialists. Her Medicaid was APPROVED because of our master plan and coordination. Soon she came to my office to catch up and she wanted to see me before she started chemotherapy. I took her back to the same conference room where we had first met. This time, it was a “meet and greet” for her cancer. I projected her CT scan on the screen and the latest guidelines regarding her cancer treatment on a large TV screen. I showed her the enemy. I said, “This is what is causing you to be short of breath.” She started to cry and said, “You are the first one to show me the CT scan and explain why we are discussing these chemotherapy agents.” Her prognosis was about 6 months with stage 4 cancer. After 3 years, she continued to play with her grand kids and was breathing better after chemotherapy and radiation treatments. Through this entire course, I told her to enjoy each day and think positive. Meanwhile, myself and her specialists will worry about what is ahead of us. That is our duty. Her job was to enjoy each day to the fullest and stay positive. Simple recipe for longevity. It worked. Cindy was a person who always wanted to be informed and be in charge the best she could. Her definition of quality of life was based on independence and maximizing time with her grandkids. I understood this not when I met her for the first time in that conference room. I still didn’t get it after several visits. But after years of walking this journey of life together, I learned a little more about her each time we visited. This is the beauty and value of primary care. Each visit, we learn. Each visit we get to understand one another a little better. Ultimately, a beautiful relationship is born. What finally took Cindy’s life was not the cancer itself. It was worsening kidney failure because of the toxicity related to her chemotherapy. She had to decide whether or not she wanted to move forward with dialysis. I spoke with her and her family the night before she passed. Together, we reviewed her options. I listened to her as she cried and shared her frustration with the sudden onset of this kidney failure. Then there was silence. I waited to say anything and allowed her words to sink in. We both knew what Cindy would decide. No dialysis. She was exhausted and pursued hospice care. Her last words to me that night were, “Dr Ahmed, you will never know how much I appreciate you.” Her daughter laid with her in her hospital bed that night. That is how Cindy passed. She was surrounded by family and held by her daughter. In peace. This is our WHY. Freedom from 3rd parties getting in between patient care and making people feel as if their insurance is in charge of their health care. You are in charge, and we have a team ready to help. Happy 4th of July. Stay blessed. Dr Ahmed To find the Pfizer, Moderna or J&J vaccines available in your area, please visit the link below. As of 04/05/21, our clinic has the J&J vaccine in stock.
As of 04/02/21, we have been notified our clinic will be receiving the J&J Covid-19 vaccine the week of 04/05/21. If you are a current patient, please contact our office if you are interested in signing up to be contacted when the vaccine becomes available to us. In the meantime, we have gathered a list of resources below offering one of the three Covid-19 vaccines currently available (Pfizer, Moderna, Johnson & Johnson). These resources include pharmacies, major hospital systems and county health departments which continue to receive vaccines in limited supply. Pharmacies 1) Walmart 2) Sam's Club 3) Health Mart Store - contact locations by phone 4) Cosentino's 5) Hy-Vee 6) The Kroger Co. (including Kroger, Harris Teeter, Fred Meyer, Fry's, Ralphs, King Soopers, Smiths, City Market, Dillons, Mariono's, Pick-n-Save, Copps, Metro Market) - contact locations by phone 7) Medicine Shoppe and LeaderNET - contact locations by phone 6) Full list of Pharmacies participating in the Federal Retail Pharmacy Program for Covid-19 Vaccine TIPS: -We encourage you to also contact pharmacies outside of your local city/county if you are willing and able to drive a little further to receive a Covid-19 vaccine. You may be able to receive a vaccine sooner this way. -Please call & ask if you can be placed on a "back-up" list at pharmacies. At the end of the day, if there are extra doses left, pharmacies may contact you to offer a vaccine that same-day instead of throwing out the unused dose and wasting it. -If you already have a Covid-19 vaccine scheduled in the future and end up receiving one elsewhere sooner, please make sure to notify your originally scheduled vaccination site you received a vaccine so they can open up your spot to others on the list. Hospital Systems 1) AdventHealth 2) Menorah Medical Center 3) Overland Park Regional 4) Olathe Health 5) Saint Luke's Hospital 6) University Of Kansas Health System 7) Kansas City VA Medical Centers County Health Departments KANSAS 1) Johnson County Kansas 2) Wyandotte County 3) Contacts for ALL Kansas counties MISSOURI 1) Kansas City 2) Jackson County 3) Platte County 4) Clay County 5) Cass County Community Vaccine Initiatives 1) Operation Safe, Clay County 2) Negro League's Baseball Museum, Hy-Vee Partnership March 28, 2021 KSHB news article VACCINE LOCATIONS KS & MO www.kshb.com/news/coronavirus/kansas-city-area-covid-19-vaccine-planner-for-march-28-april-3 TRACKING THE VACCINE: KCTV5 NEWS APP ALERTS FOR SMARTPHONES KCTV5 News has a free news app that has Covid-19 Vaccine alerts which will notify you of appointment openings in Kansas & Missouri. Please download their app to stay-up-to date on openings by clicking here: COVID-19 VACCINE ALERT NOTIFICATIONS Yes! It is true, I found love. It is so beautiful. Magical. Direct primary care.
Of course, I am trying to be humorous here. Before people lose their minds, yes, my wife, Arshia, is my other true love ;-). She manages it all and puts up with my crazy ideas. God bless her. I am still amazed how she agreed to support a scrawny kid waiving his old school medical bag and yelling "I'm mad at this health care system and I am gonna show people a better way to do it!" 2020 was a challenging year for all of us indeed. BUT, I always look at challenges as lessons. Sometimes in life we are not ready for the things we want to do and life throws challenges at us to get us ready for big endeavors. These lessons make us stronger, more creative, and more informed. In 2020, due to the Covid-19 pandemic, we saw millions of Americans turn to their tablets, phones, and computers to visit with their doctors. The country all of a sudden started practicing direct care! Medicare changed its rules and said use ANY video conferencing ability, including FaceTime to visit with your doctor. Use whatever! Hmmm, I remember screaming this back in 2014 holding my rugged medical school bag, wearing roughed up scrubs, and doing house calls with this crazy idea! I was already doing telemedicine visits prior to the pandemic and my patients and I became even closer this year. We struggled together. As an Internal Medicine physician and Hospital Medicine specialist, it is so rewarding to manage the chaos in the hospital. But, to take care of people through various settings including the outpatient clinic, long term acute care hospital, assisted living, and finally home is the most rewarding experience. To see someone who was in the hospital for an acute COVID-19 pneumonia for more than 50 days with a trach and feeding tube come off the assistance of a ventilator and literally walk to their car on discharge day at our long term acute care hospital is the best feeling in the world! At LiveActive Primary Care, we have accomplished something really significant. Direct Primary Care is a mindset, attitude, a philosophy. It is not just a way to practice medicine in an office and go home at night. No. It is more than that. We take this attitude and mindset of preserving the sacred relationship between physician and patient and apply it to ALL settings of health care. We intend to show the world that direct primary care influences ALL aspects of care in our health care system. It means we do not allow third parties to dictate what care someone gets. It means we get creative. We tie loose ends. We create game plans. We communicate with the entire team of people who will help someone live their best quality of life. It means breaking down silos and leveraging each of our talents to serve our community at the highest level. Our team has grown quite a bit in just a few months. We demand 2 things when we are approached by someone who wants to join our team. One, you have to smile and laugh...genuinely! Two, you have to have passion for what you do and be willing to take your talents to the highest level. No fear. Our organizational philosophy is that each one of us brings unique talents and experiences and we should respect that. If we allow it to thrive and be challenged, we all benefit from the exceptional service that is created. We do not allow any barriers to get in our way of providing the best care to our community. So, going into 2021, we are preparing to take our attitude of direct primary care even further. Currently, we provide services in assisted living facilities, hospital, long term acute care hospital, our office, and at home. There is more work to be done. Why can't cardiology or pulmonary services provide direct care? Why not? Why can't we eliminate readmissions to hospitals for things that can be managed by hospital trained providers in the community? Can hospital services be done at home? Why not? Why are there soups of specialists in complex cases? Do we really need to have so many specialists involved? Are we treating to optimize quality of life or padding statistics or did we forget to even understand a patient's definition of quality of life before we even started a treatment plan? So much more to come... If you or a loved one would benefit from our love for direct primary care, JOIN US! To enroll, click on the link - JOIN NOW. A sincere thank you to all my wonderful family, friends, colleagues, dear patients and their families for your continued support and trust. Here is to a blessed and healthy 2021! Your physician, Dr. Haseeb Ahmed After months of fighting this virus in the hospitals, I cannot tell you how excited I am to see the amazing work our researchers have done since the start of this pandemic. You have to remember, this is a worldwide pandemic. So, we learned from one another across the globe. This experience demonstrates how we all are unified in this vulnerability. As a physician, I remember feeling the pain the people and the health care workers were feeling in Italy, Brazil, UK, and of course here in the US. We lead the world in the total number of deaths due to COVID-19. Personally, it has been exhausting. I have never signed so many death certificates in my 13 year career. I have never cried as much as I did while listening to someone's heart and lungs who was infected with COVID-19. It is so hard to see a chest x-ray or CT chest of an infected patient who initially might be smiling and talking to you but deep down you know that in the next few days you will be battling a virus that will bring all its might against this same patient. So many sleepless nights have passed with worrying about people under my care and crying over those who I lost. Many people may not know that as a physician who is treating a COVID-19 infected person in the hospital, you get to really know their family members and their stories as these cases require long hospital stays. Hearing the struggles of others whether it is economic, social, or other issues makes the whole situation even harder. To say the least, it has been very difficult. I smile a lot so people may not ever know the pain or exhaustion I feel as I write this blog. But, I do this work because I am blessed to be in a position to heal. I am blessed with a team of nurses and nurse practitioners at LiveActive and all the team members we have at our assisted living facility, hospitals, and long term acute care hospital. Together, we have lifted each other when we were down, worked extra shifts when we could, and our families took on risks as we fight this virus. Please thank the spouses of health care workers too! I feel that we do not recognize them. They are the ones who fear daily for their loved ones. It is they who may have had to make us smile, give us a hug when we needed it the most, or put their concerns on hold while they lend us their ear as we share our frustrations and stories. BUT...we finally are getting close to vaccination! Here are some important points to remember. The CDC website is helpful, but I found it a bit much to navigate through and make sense of so here is my attempt to simplify it for you. What the heck is a mRNA?We are all familiar with DNA (deoxyribonucleic acid). This is the molecule that contains the genetic code for organisms. Remember, plants, bacteria, and many other organisms have DNA. So to get from the genetic code to actual protein synthesis, messenger RNA (mRNA) is needed to transcribe the code for production of protein. So, how does a vaccine take advantage of this process?COVID-19 mRNA vaccines give instructions for our cells to make a protein called “spike protein.” This protein is found on the surface of the virus that causes COVID-19. Where do you inject the vaccine and how does it work? Once it is injected in the upper arm muscle cells, our cells use the mRNA to make the “spike protein”. Our immune system then goes into action! It recognizes the protein as a foreign invader and starts to build an immune response and making antibodies. Not only will our body protect us from the virus this time but also against future infection. How safe is the COVID-19 vaccine? To answer this question, you must understand how a vaccine is developed. Here is a simple picture without getting too technical. At each phase, researchers assess safety while increasing the number of subjects involved in the studies. 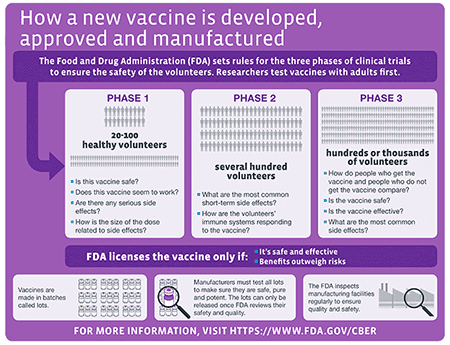 In addition, the FDA also looks at the manufacturing of the vaccine to assure its safety. Manufacturing companies must seek permission to market a vaccine for use in the United States. If the FDA approves it, there is continued monitoring for safety and effectiveness. There are various surveillance systems in place that assist in monitoring for safety and effectiveness. The CDC website has some great information but it can be confusing. Here are some quick facts that is from their website: Facts about COVID-19 Vaccines (cdc.gov)
Which vaccines are currently in PHASE 3 Clinical trials? As of November 24th, here are the current vaccines in progress or being planned:
This sounds great, but how much is it going to cost me? Per the CDC website, vaccines purchased with US taxpayer dollars will be given to the American people at no cost. Vaccine providers will be able to charge administration fees for giving or administering the shot to someone. This fee can be reimbursed by the patients public or private insurance company. If uninsured, this fee can be reimbursed by the Health Resources and Services Administration’s Provider Relief Fund. So, should I get it?In my humble opinion, I think you should. I trust our country and our researchers. I trust the FDA process. I have faith that every study has been and will be conducted with the utmost care and thoroughness. The FDA is notorious for being complete and having a rigorous process when approving new treatments.
Please discuss your concerns with your primary care physician. Review the CDC website. Ask questions. Stay safe. We all have become stronger and more informed as a result of this terrible pandemic. UPDATED 01/12/2021: With Missouri and Kansas in the initial phases of their vaccine distribution plans, some counties are allowing residents to sign up to be notified when they're eligible. This is a great new article that lists how to get on the Covid-19 vaccine list for certain counties: https://www.kcur.org/health/2021-01-12/kansas-city-heres-how-to-reserve-your-spot-in-line-for-a-covid-19-vaccine?fbclid=IwAR15z4Ni9FLxqrDbn8r_omTqYVUGcfUlFtT1jmz9F6Ec9tunLEO0xnF-Fv4 Your physician, Dr Ahmed  Heather, RN Heather, RN Hey guys! Nurse Heather here. For those who don’t already know, I am a licensed and registered dietitian. Yep, you read that right – nurse and dietitian. Weird, right? And to answer your question, no, it was not my original plan to take that career path.
I first obtained my bachelor’s degree in dietetics from Iowa State University and went on to complete my dietetic internship at the University of Iowa Hospitals and Clinics. After graduating and obtaining my license and registration, I worked in long-term care and acute-care settings. I loved interacting with and educating patients! As time went on, I found myself wanting to do more for my patients than my degree allowed – I wanted to impact more than their nutrition, I wanted to provide hands-on care, and I wanted more opportunities to build a deeper connection with my patients. *Insert nursing school here.* One quick year later, I had my second bachelor’s degree, this time in nursing, from MidAmerica Nazarene University. Long story short, I am grateful to be in a unique situation now where I get to utilize both my nursing and dietetics degrees. I do enjoy nutrition, and I believe it is the foundation to healthy living – that is why I am excited to start offering nutrition sessions to our members in the near future! As we work out the kinks, I plan to occasionally post nutrition-related tidbits here, so stay tuned for some healthy insights as we start navigating the holiday season! |
Author"He who studies medicine without books sails an uncharted sea, but he who studies medicine without patients does not go to sea at all." Archives
March 2023
Categories
All
|
 RSS Feed
RSS Feed
We are passionate about practicing medicine
|
|
CLINIC HOURS
MONDAY 9am-5pm TUESDAY 9am -5pm WEDNESDAY 9am-5pm THURSDAY 9am-5pm FRIDAY 9am-12pm Closed 12pm-1pm daily for lunch SAT&SUN CLOSED |
2024 Holidays - CLINIC CLOSED
New Year's - January 1st Memorial Day - May 27 Independence Day - July 4 & 5 Labor Day - September 2 Thanksgiving - Nov 27, 28 & 29 Christmas - December 24, 25 & 26 |
Contact Us
Tel: (913) 549-3884
Fax: (913) 273-3343
Email: [email protected]
6650 West 110th Street
Suite 220 A
Overland Park, KS 66211
Fax: (913) 273-3343
Email: [email protected]
6650 West 110th Street
Suite 220 A
Overland Park, KS 66211