|
In this final blog post as part of this series, I feel the need to start with illustrating the difference between Direct Primary Care and Concierge Medicine. It is very important for my readers to understand the terms we are using in explaining how Direct Primary Care in combination with the Affordable Care Act (ACA) is the best solution for our healthcare system. In addition, I refer to direct primary care as well as direct medical care in general. I strongly believe, as many specialists, surgical centers, and endoscopy suites do as well, direct pay for medical services is less expensive than billing to insurance companies. 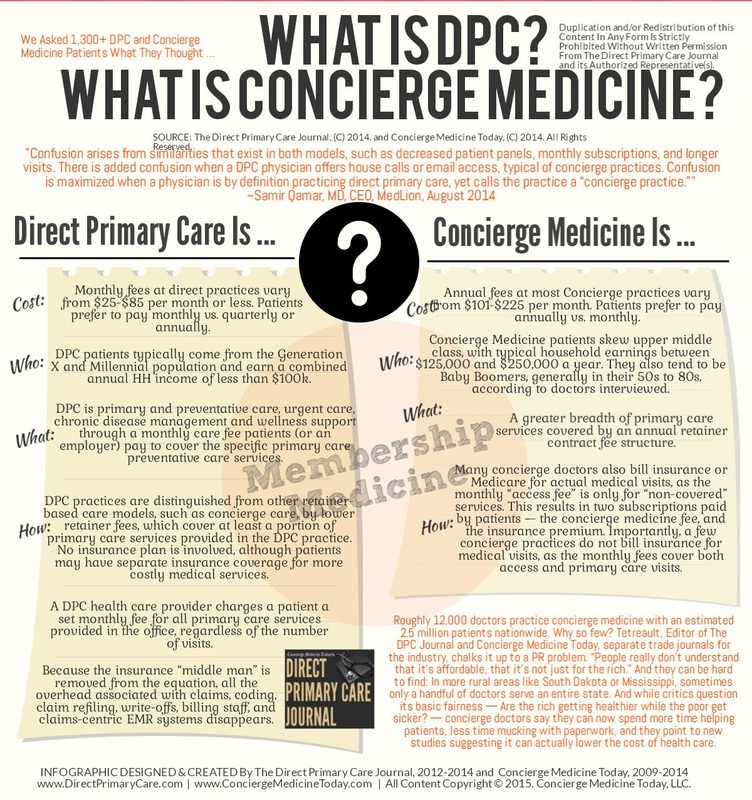 So, in summary, Direct Primary Care:
Current Situation
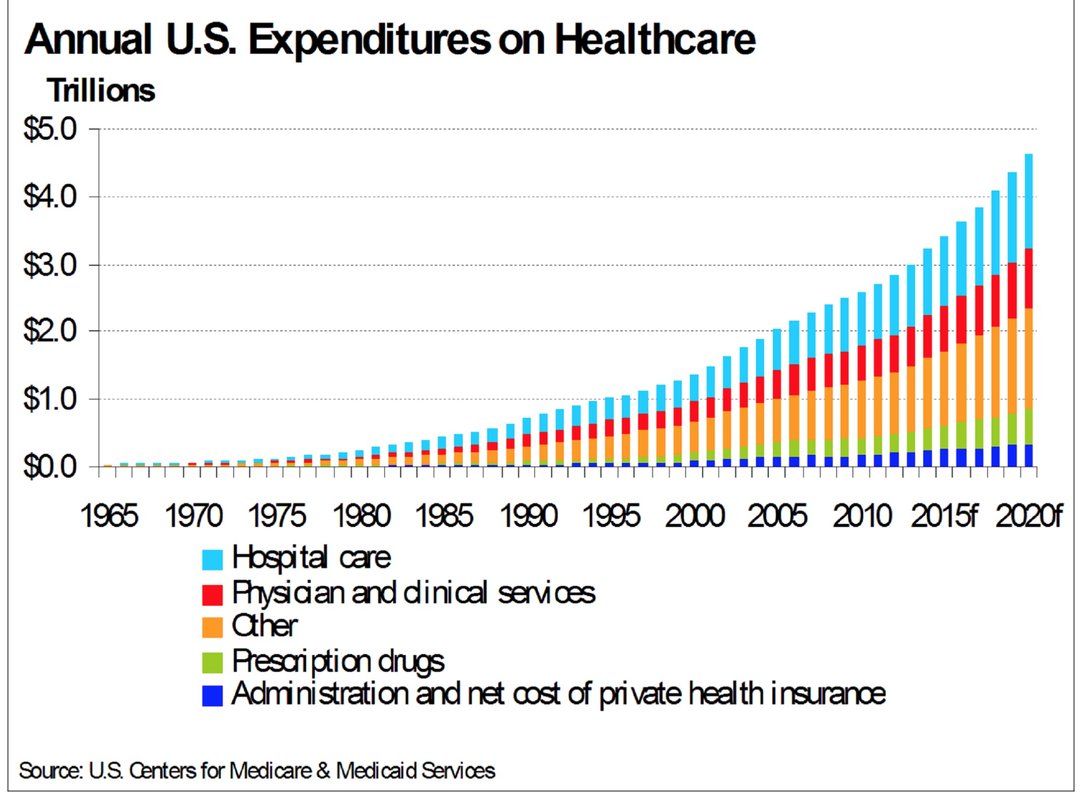
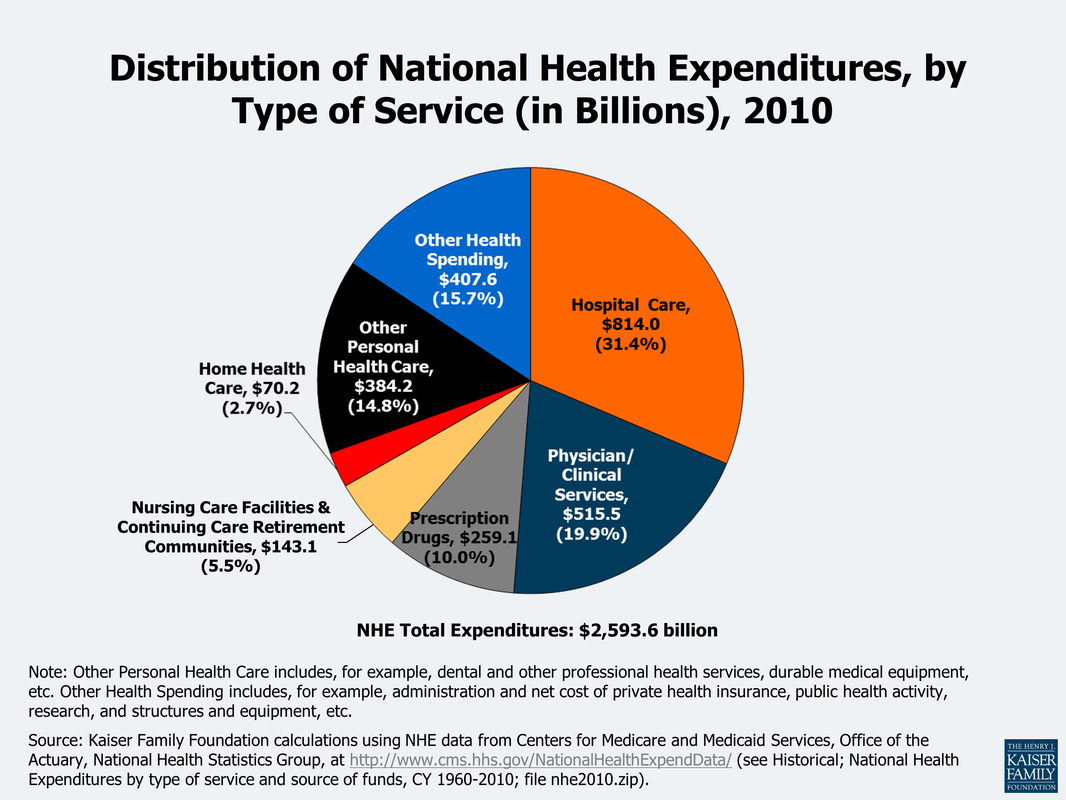 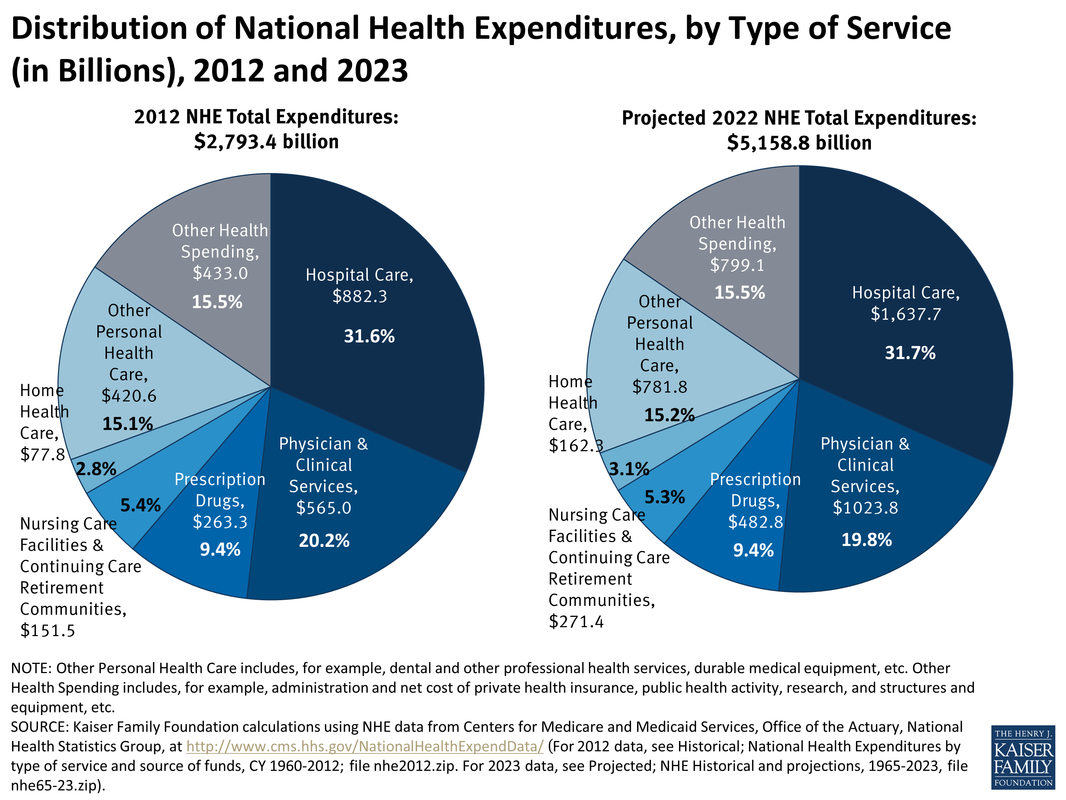 In order to really understand the economics of health care spending on a national level, think about this: We spend about 25% of the national budget on four health insurance programs — Medicare, Medicaid, the Children’s Health Insurance Program (CHIP), and Affordable Care Act (ACA) marketplace subsidies. How efficient are we with our tax dollars? What is the return on our investment? We spend 17.2% of our GDP on healthcare; more than any other nation in the world. Take a look at the graph below. We spend 49% from public funds on health care. The reason for inefficiency all of a sudden becomes more clear. 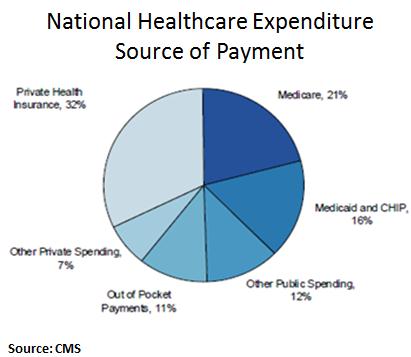 What happens when direct care and health insurance programs work together?It is estimated that about 80-90% of all health issues can be resolved or prevented in the primary care setting. Yes, you read that right, a significant majority of issues can be managed and prevented in the office. Urgent cares, stand alone ER, and now the new trend of small hospitals are feeding off the need for accessible care. Large health systems are trying to reach more patients with multiple "footprints" across the region to bring in more people into their system. People find comfort in that all their information is "in one place." But, we tend to forget that when physicians are on medical staff or teach at various hospitals, we have access to the EMR and able to coordinate hospital care, like the "old" days. I would argue, when your patient panel is smaller (less than the traditional 6,000 patients) then it becomes easier to coordinate and provide hospital care. Economics of direct medical care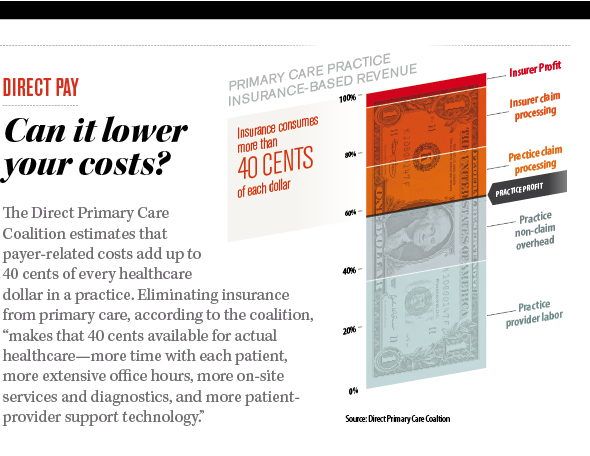 A. Consumers save and decrease out of pocket expenses By saving $0.40 on the dollar, practices are able to offer more services, use technology to make themselves available to their patients, while keeping the cost of their services low. The consumer's out of pocket expenses are drastically decreased as majority of direct primary care practices do not charge co-pays or any additional costs for in clinic procedures. In addition, the discounted imaging, labs, and medications are drastically lower than with insurance. B. Health insurance premiums will decrease drastically When we take insurance companies out of the outpatient world: all primary care practices, specialty office visits, imaging, laboratory, physical therapy, occupational therapy, speech therapy, and some outpatient procedures, then the insurance companies are purely covering inpatient care and catastrophic care. A large component of insurance premiums are to cover these services. So eliminating the outpatient services will significantly reduce these premiums. The medical offices, imaging centers, laboratory facilities, and many procedural suites save big when they don't have to bill insurance by reducing their staffing, paperwork, and resubmitting of claims. Thus, the cost of their services will come down and the market is open to competition. Accounts receivables have minimal to zero balance; leaving liquid cash in the bank to offer more services. Please note, many endoscopy suites, surgical centers (like Surgery Center of Oklahoma) specialty offices, imaging centers, laboratory facilities, and of course primary care offices are moving to a direct model because of these benefits. C. Cost of hospital care and need for more services will decrease With accessible and affordable primary care, studies have shown that not only do people visit with their primary care doctor more, but their risk for admission to a hospital is drastically lower (see diagram below from our friends at Qliance). Hospitals have an opportunity to embrace a direct model as seen around the world and surgical centers where there is no insurance billing. But, I fear this will take some more effort and health insurance lobbyists are quite powerful. So, I will push the envelope towards at least getting the outpatient world out of the grasps of health insurance. 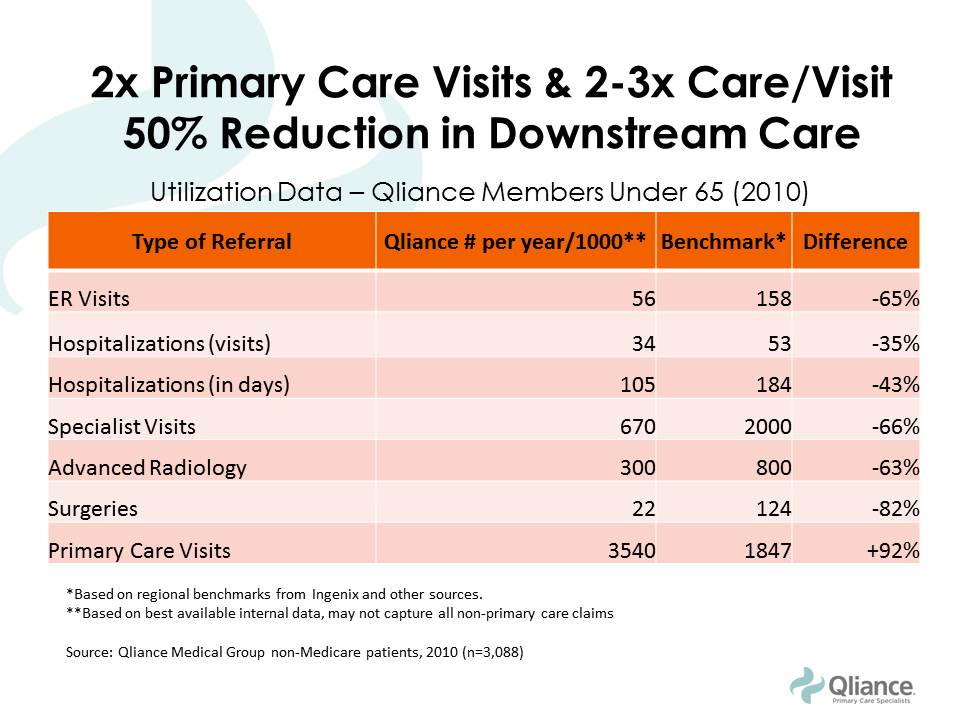 D. Federal health spending and taxes (Federal and State) will decrease Medicare and Medicaid are government sponsored health insurance programs that will also be focusing on inpatient and catastrophic care in this new model. Folks who are paying lower premiums can fund their Health Savings Accounts (HSA) or Flexible Spending Accounts (FSA) to pay for direct medical services. These are pre-tax dollars and funding them is more realistic as the consumer will be paying less out of pocket for their health insurance premiums. Even the $50 monthly fee for direct primary care can become difficult for some Americans. This is where practices should be given a tax incentive to provide free charity care. The more they do, the more they save. Currently, tax laws place a cap on how much they can claim as charity care. Each practice can also be allowed to set up a charitable foundation and reduce the complexities of forming of 501(c)(3) organization. This will enrich a community feel of delivering health care and bring all Americans together in providing quality care for one another. States can expand Medicaid without having to increase their state taxes as much. The IRS and the ACA must agree on terms, as they currently have different definitions for HSA and FSA as to what qualifies as a medical service. This will happen soon, but in aligning the definitions, this will incentivize more development of direct medical practices across the country. So, what does it look like for the consumer purchasing medical services?To answer this question, lets put ourselves into the shoes of a imaginary 40 year old man named Tommy. Tommy is a car parts salesman and recently took over his fathers business. He is very energetic and overweight. He has diabetes, heart disease, and some kidney disease. He starts searching for a direct primary care doctor in his area. After spending time meeting the doctors and their staff at different practices, he settles on one. We can call it LiveActive Primary Care www.liveactivepc.com He then looks for a health insurance product that has his hospital of choice in their network and co-incidentally his new direct primary care doctor also provides hospital care at that same hospital. What a find! His premiums are much lower and he gets a plan with a HSA account so he can fund his card with pre-tax dollars. His first visit with his direct primary care doctor is 60 minutes where all his health issues are discussed and a plan of care is developed. He walks out with all his labs done for less than $35, medications that are significantly less, and plans to see his kidney specialist soon. Since his kidney specialist does not bill insurance, they are able to see him same day or next day. All his doctors are a text message away. When he arrives at the kidney specialists office, his case has already been discussed by his primary care doctor and the specialist. This is a real possibility as both of these doctors have the time to discuss cases instead of seeing 30 patients a day with unnecessary paperwork. They discuss the case and he is on his way home with a plan. When Tommy goes to the hospital, both of his physicians come to take care of him. The nurses and hospital staff are ready to take care of him upon his arrival. How about the consumer with no health issues?So for this part, we meet Elon. He researches a direct primary care practice just as Tommy did and signs up. His health insurance product is just as cheap as Tommy. Elon is playing with electric cars and hurts his hand. He texts his direct primary care doctor with a picture of his swollen hand. His doctor takes a look at the picture and calls him to discuss his symptoms via video chat. After assessing his mobility, Elon is told to get a hand X-ray, which costs less than $40. Elon walks into the imaging center, gets his X-ray done, and within minutes his direct primary care doctor calls him to say that they saw the images and he needs a cast placed. Elon is told to come the office that same day and a cast is placed for $40. Elon goes back home to play with rockets. How will hospitals save money in this health care system?The ACA attempts to improve quality of care by penalizing re-admission rates, in hospital infections, and pushes for a medical home model. With the development of various direct care practices, the consumer is able to create their medical home: pick their direct primary care doctor, pick which specialist they like, and hospital. The hospitals should see less readmissions as the care in the outpatient setting is more accessible and affordable. There is a reduction in risk for hospital acquired infections with decrease length of stay. The Emergency Rooms will not be overflowing as patients are able to be seen by their direct primary care doctor quickly or in their home as needed. If someone does have to go to the ER, then the process is much more efficient. The primary care doctor and the ER physician have already talked about the case so upon arrival of the patient, care is started immediately. SummaryThe ACA has more than 33,000 pages of regulations. Remember this famous photograph in the Washington Post: But there are several benefits that should be continued:
Changes that need to be made to the ACA:
Now, this solution is a key ingredient in decreasing our national expenditures quickly. But, it is not complete on its own. We must make continued efforts in reducing pharmaceutical cost as well as medical devices. This will take some aggressive regulations and encouragement of free market. As the insurance companies remain involved in hospital care, long term care, and some other services under the model, there must be efforts to make billing more efficient and decrease the amount of waste we produce as discussed above.
Finally, as a country, each American must make a commitment to improving their health. We can open several doors for the American people, but as many direct primary care physicians will tell you, despite all these resources and at times FREE medical services, we still have trouble maintaining compliance in some of our patients. This must change. It will take comprehensive effort to improve our national health care. President Obama, despite your opinion of his presidency, has ignited the push towards better health care for all of us. It is on us to keep pushing, improving, and supporting programs that have intentions of providing accessible and affordable care for all. Dedicated to my beloved fellow Americans, Dr. Ahmed
3 Comments
This is part 2/3 of My prescription for better health care for ALL Americans.  With the new president-elect nominated by the American electoral college, there are increasing worries about repealing the Affordable Care Act (ACA). Is it possible to repeal such significant legislation of our time? Will millions of Americans lose their insurance coverage? Since its inception in 2010, an estimated 20 million of the estimated 47 million uninsured Americans gained health insurance coverage with surveys pointing towards many satisfied customers not only with their plan but also their chosen doctors. Studies, as cited by the Common Wealth Fund, also suggest an improvement in quality of care as a result of ACA implementation. In the last 6 years, there has been increasing interest in multi-payer initiatives to promote quality primary care by reimbursing physicians a set fee per member of their practice (sounds like the government likes direct care but won't admit it). All this sounds great, right? So what is all the fuss about?Well lets look at what this "coverage" means for the average ACA enrollee:
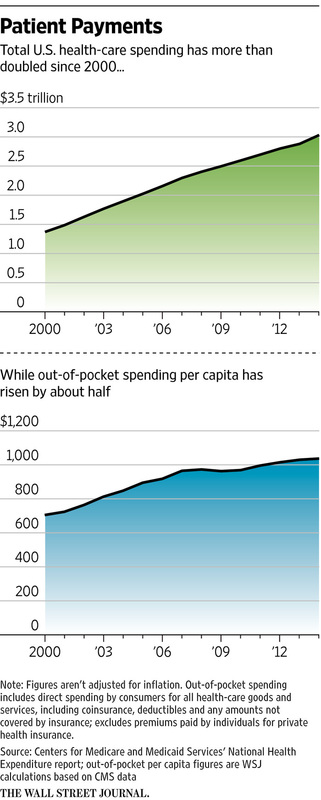
Think about this: When a person gets admitted, the hospital staff runs them through a myriad of exams and tests quickly to maximize their revenue (initial evaluation is highest paid with decreasing reimbursement for follow up visits), and then discharge them to the clinic setting where the wait times are long and the patient has little time with the doctor. The social workers and case managers will be the first to tell you there are several moments during a hospital discharge, we can predict someone will likely come back (called LACE score). To add to all this chaos, add the fact that the insurance companies will deny medications that at discharge might be needed or imaging that is needed for follow up. Hey, but I have coverage, right? Delay in care with prior authorization and denial of medications is what only the American who experiences this in some way truly understands. Health care is a $3 trillion industry. Each change in policy means millions of dollars worth of changes in staffing and organizational structure for hospitals. Like any other business, these costs will need to be recovered in some way. Thus, the rising hospital bills, avoiding certain payers completely, and entertaining providing services in a cash basis without involving insurance; it's so much cheaper! Health insurance adds about 5 staff members for each physician with denial of claims about 15-20%. Accounts receivables increase as the facilities await payment while continuing to pay for billing services to resubmit and submit new claims. This is the single largest cost and waste in our health system. From direct costs of paper, printing, software and hardware, billing services, to indirect costs of time wasted, prior authorizations, insurance denials and requests for more forms, less patients seen due to paperwork, and burn out. This is the foundation for the need to see 20-30 patients daily to capture a reasonable revenue stream to keep the business running. More on this in the final blog post. Enter direct care. The American Academy of Family Physicians (AAFP) proudly supports direct primary care and holds the single largest conference in Kansas City, MO every year. This single event has grown from a few 100 to over thousands of attendees, including physicians, medical students, medical residents, technology vendors, and others who are eager to partner with direct care practices across the nation. Their tremendous support stems from the growing national shortage of primary care physicians, increasing prescription medication costs, poor access to care, and unaffordable medical care despite insurance coverage. The American College of Physicians (ACP) has also written a white paper on practices contracting with their patients instead of insurance companies. This paper has increased the conversation differentiating direct primary care from concierge care. A social media storm was lead by yours truly. Sorry ACP, but I cannot tolerate poor research prior to writing a paper. SummaryHere is the reality:
Solution
How would this new health system look like? I discuss this in my final blog post for this 3 part series.
Cheers! Dr. Ahmed My prescription for better health care for ALL Americans. Part 1/3: Top 5 factors raising premiums11/7/2016 Introduction Those of you who follow my blog know the foundation of my leadership philosophy. Empower your team with tools and resources they need to solve problems creatively; ultimately bringing success to the entire group. First step in solving any complex issue is to first understand the problem. And so, we start by looking at the problem in the economics of delivering care by understanding the cause for rising insurance premiums. I hope to raise your awareness in this 3 part series to illustrate the real issues with the Affordable Care Act and propose a solution which I think will propel us to being the most innovative and efficient health care system in the world. If you are like most Americans, the open enrollment season is confusing, nerve-wrecking, frustrating, and quite honestly, an overwhelming time. How do you choose which insurance is right for you? All the language and terminology is so confusing that making sense of a single plan is a daunting task. Insurance brokers are there to help, but the industry is changing for individuals at least as the insurance companies are not paying these brokers commission for selling their product; leading to less brokers out there helping individuals and families. Naturally, we wonder why the premiums are so high and why they keep rising? Here are the top reasons why insurance premiums are rising and will continue to rise until we finally agree to privatize primary care and other outpatient services; keeping health insurance out of these basic services. Top 5 factors
  How has the rise in insurance premiums compared to median household income or earnings? 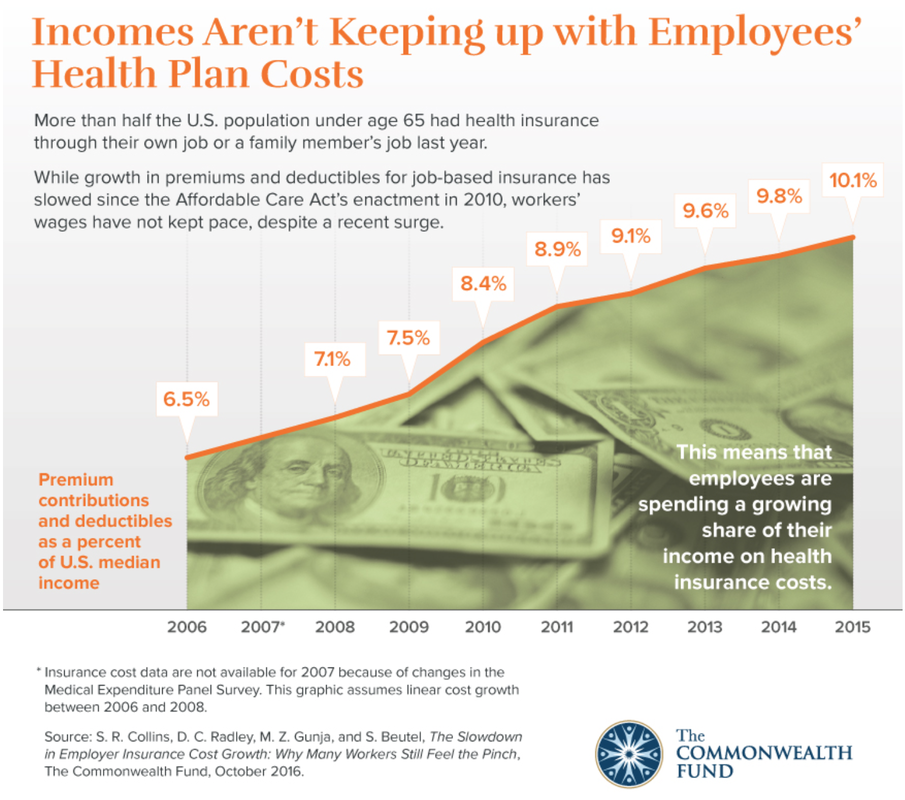 So, to put this in perspective, workers are not earning enough to keep pace with rising insurance premiums. This leads to either the employer spending more on health care coverage, letting go of some employees in order to provide coverage for others, downsize the business, or stay less than 50 employees to prevent having to require health insurance. This de-incentivizes economic growth. How does this make any economic sense? Higher premiums mean less out of pocket? Wrong!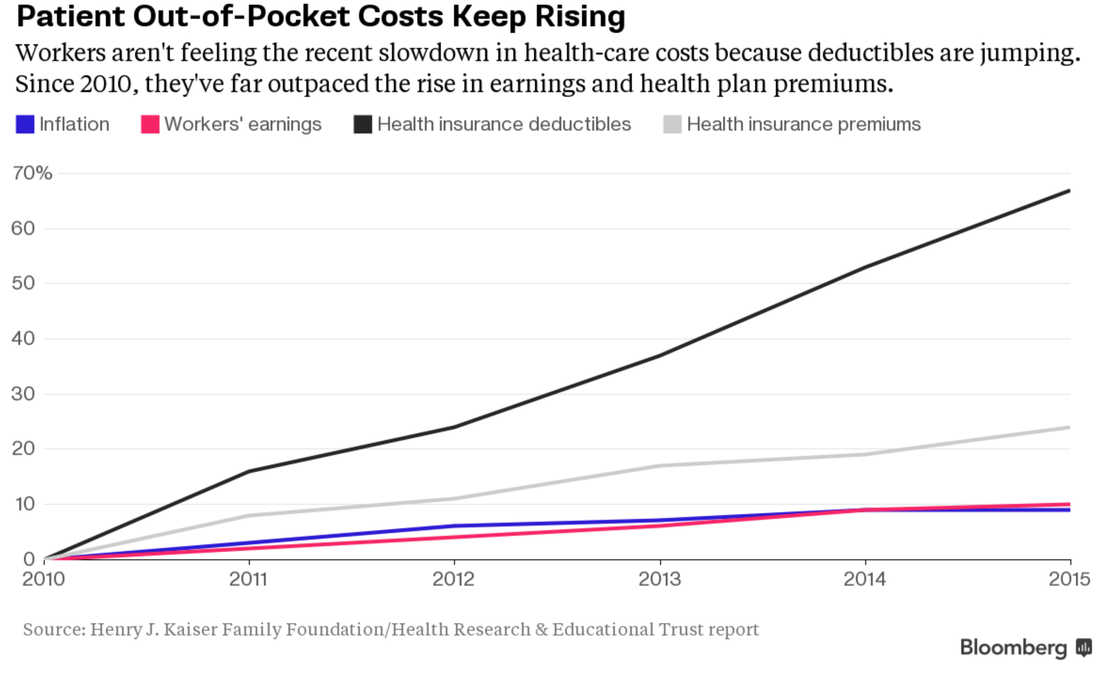 Your analysis is correct: rising premiums and deductibles are outpacing inflation. This is why earnings are not keeping pace with premiums or deductibles, causing Americans to hold onto their wallets even tighter. Rising Chronic Illness leading to higher costs of care 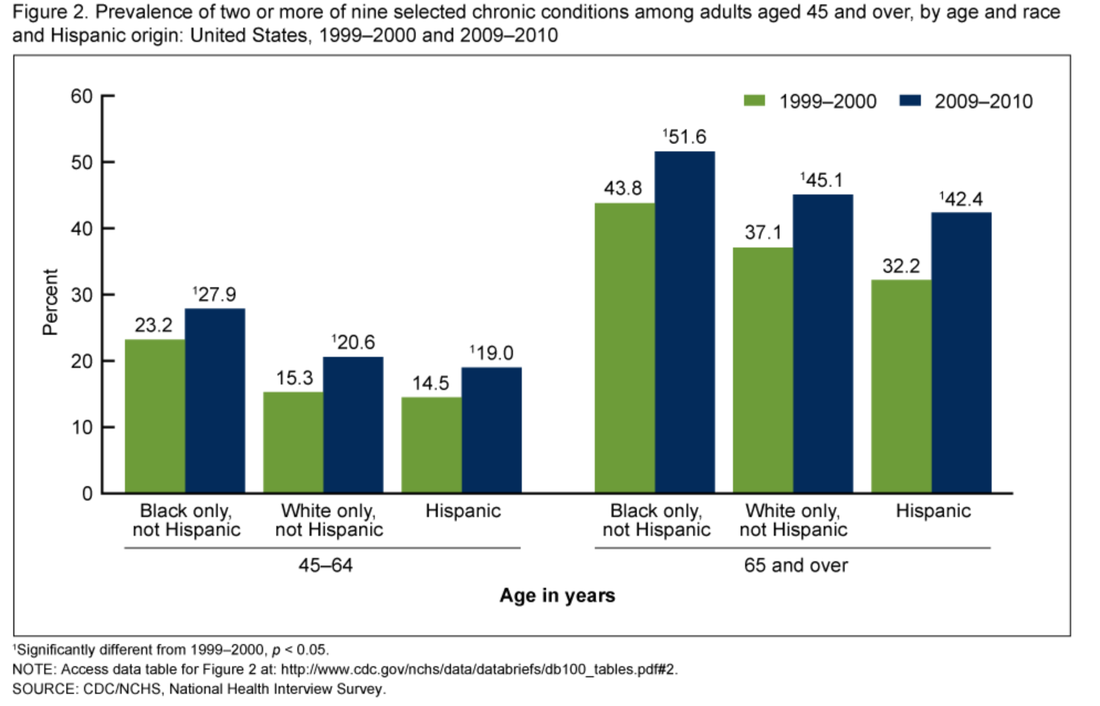 This is the reason why investing in primary care is so critical to keep costs down. More chronic illnesses does not necessarily mean more specialty care. Primary care is built, conditioned, and positioned to be fully capable of managing these illnesses at a low cost. The problem arises when the system does not allow primary care to do what it is capable of offering. Instead, the system encourages more specialty care. Even with value based purchasing and the movement towards rewarding value rather than volume, the cost of doing business in health care favors larger health systems instead of small private practices. Ultimately, making no progress in making the delivery of health less complicated, more personal, accessible, and affordable. Will the demand be met with a supply of primary care physicians? 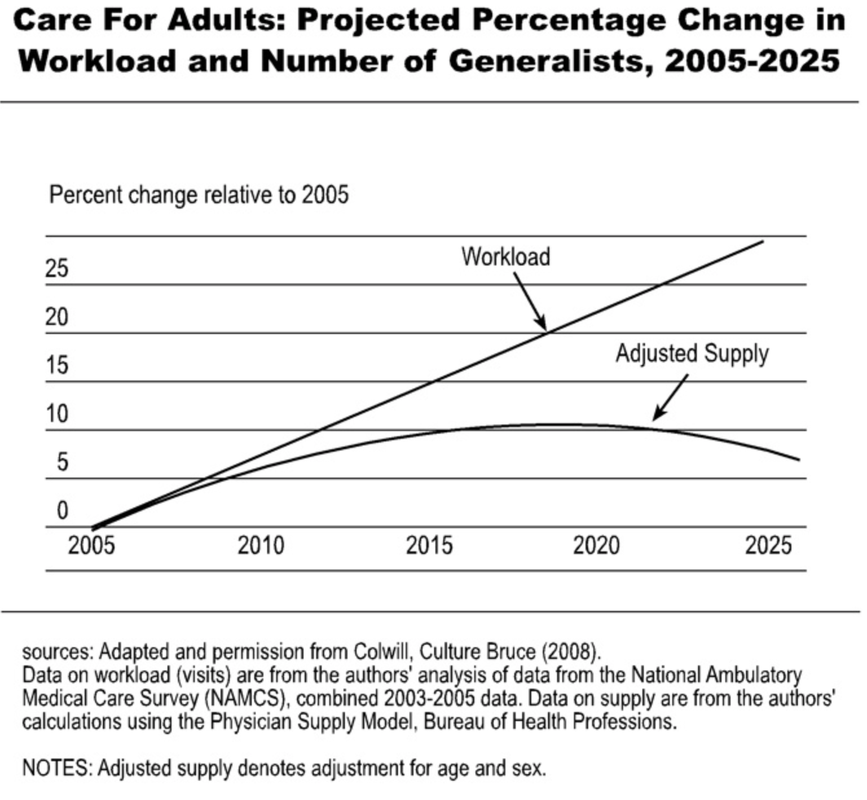 The current health care market is ripe for future primary care physicians. Many may look at the current state of primary care and run away. But the informed and astute medical student will understand the industry and market trends illustrated in this blog and realize this is the best time to be a primary care physician. It is also a wonderful opportunity for investors and innovators to assimilate modern technology with quality primary care. No, not telemedicine by itself. The human touch and relationship must never be obliterated. Imagine the patient experience with modern technology and medicine that focuses on building strong, long lasting, relationships.
That is the future of primary care. That is the future of the United States Health Care System. If you are a investor, innovator, or someone in the community who wants to support my vision, please support our growing practice. Health care will be much different and more efficient for the next generation. Dr. Ahmed Have you ever wondered how this prescription drug abuse epidemic spiraled out of control? How did we let this happen? Who are the major stackholders? These powerful drugs were developed with a real noble purpose, but soon cycled out of control. Was it our own doing? Similar to cigarette companies, pharmaceutical executives have become significantly rich at the expense of bringing incredible harm to all of us. This is our terrible reality across all industries - greed always results in harming everyone involved. Physicians have been screaming about the dangers of these medications, but lawmakers continued to ignore them Why do we do this? Ignore the scientific community for the mighty dollar. Whether it be the approaching epidemic, rise of harmful medications or technologies, or gun control - the concern for financial profits always win. The commercial manufacturer of morphine started out in Germany in 1827. In fact, morphine was the painkiller of choice during the American Civil War. Interestingly, the doctor who invented Coca Cola formula had developed a morphine addiction during the Civil War and in their attempts to solve this issue, cocaine was sought. The new drink had cocaine mixed into it and sold to a pharmacy in Atlanta. During that time, this was perfectly legal. Heroin was created by Bayer Company in Germany in 1898. It's sole purpose was to be a remedy to the morphine addiction. Legislation, like The Pure Food and Drug Act of 1906 and Harrison Narcotic Tax Act in 1914, brought these addictive substances under the control of physicians; preventing casual distribution of these products. The current problem:
  Factors that contributed to such growth:
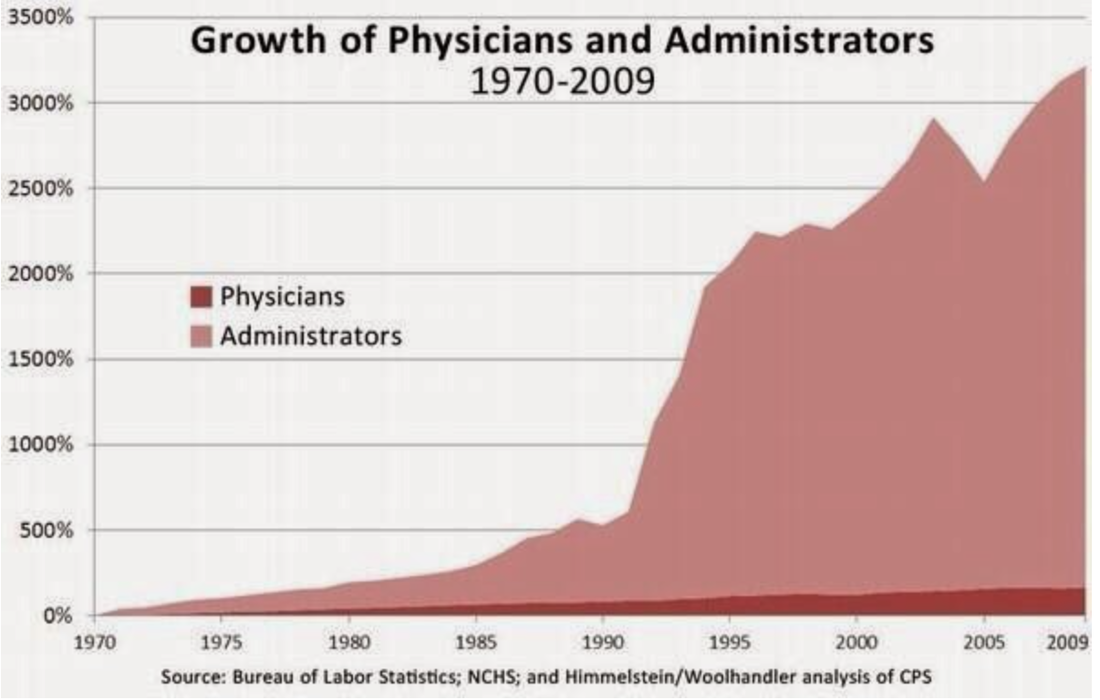
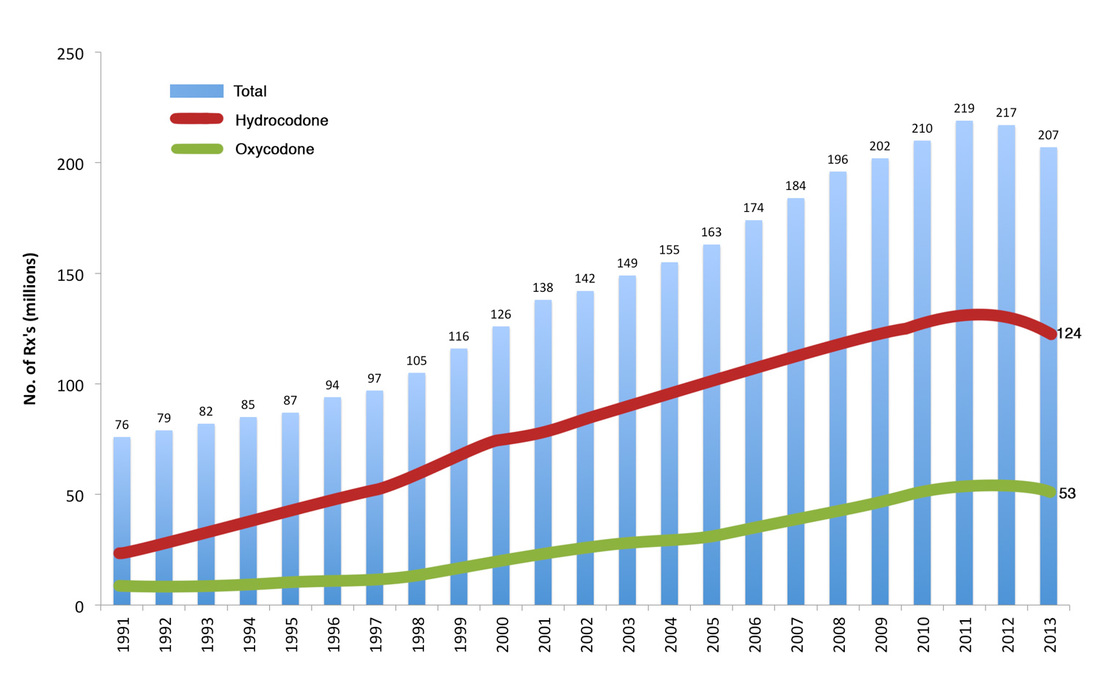
The number of prescriptions has increased from 76 million in 1991 to nearly 207 million in 2013. The United States is the biggest consumer globally. What does it mean for the pharmaceutical companies? It means more than $35 billion in sales since releasing medications like OxyContin. Annual revenues are about $3 billion for pharmaceutical companies selling prescription drugs. So, what does all this mean? Well, let's see... A medication or family of medications whose sole purpose was to help the soldiers during war starts to be sold unregulated to people around the world. Then as addiction starts to develop and people take notice, regulations are made to help control its spread, but either inadvertently or not, products like cocaine and heroin are used to "remedy" the situation. This leads to more addiction. Crap! Meanwhile, the US health system was undergoing major changes. In attempts to control costs in the 1960s-1990s major developments in public and private health plans were developed. Not too surprisingly, as the managed care organizations were attempting to control costs, US health expenditures started to rise, while reimbursement started to fall. Pharmaceutical companies started to market heavily and capitalized on a health care system that was reducing clinic visit times to an average 7-10 minutes, which led to more written prescriptions. Sound familiar? Our country has a HUGE antibiotic resistance problem where antibiotics are prescribed unnecessarily. The American public doesn't see the "super bugs" which claim many American lives where these bugs are resistant to ALL available antibiotics. Pharmaceutical companies do not invest in making more antibiotics as there is more money to be made in drugs that are taken for a long time, instead of the 5-7 days regimens that are usually prescribed for antibiotics. But, we digress. So what does the US government do to fight this epidemic? Spend more money where it doesn't matter! The President signed legislation that authorizes $181 million a year for new programs to train emergency personnel in administering drugs to reverse opiod overdoses and help communities purchase those drugs, as well as develop treatment and overdose programs. This means that pharmaceutical companies have more buyers for medications like Narcan and other products. Which leads to more profits! These treatment centers will be overwhelmed with the large demand as the public now has available "quick reversal" agents. This sends the wrong message and does NOT get to the root of the problem. Those of us who have taken care of overdose patients know that the problem does not cost so much money, development of more "reversal" agents, nor does it require capital investment to create "treatment facilities." The solution is simple: Establish a human connection involving time to talk, engage, motivate, build strong relationships, and bring people together. What does this solution look like more specifically? All physicians, including specialists, are demanding better primary care. Longer visits allow for conversation and developing a plan that may include various pain control options outside of prescription medications. The primary care setting is the place where opioid management should take place. Why not? The primary care physician is the leader of their care; the quarterback who is most likely or should be managing multiple health issues. They are the ones who spend time with the family, loved ones, might even have done a few house calls, knows what barriers exist to better health, and is the one making referrals or partnerships to bring more solutions to their delivery of care. This is what true primary care looks like. Not a place to get a referral to a pain specialist or some methadone clinic. Why do we accept such nonsense? Let the primary care doctor to what they are trained to do. The health system must support and allow this interaction to happen because this small investment will prevent huge costs in the future. Psychologists, counselors, psychiatrists, social work, and others might need to be involved. More importantly, there cannot be a delay in seeing each of these specialists and there needs to be total - 24/7 - contact between physician and patient to prevent "loss to follow up." This solution is cheaper, preserves human dignity, and most importantly it gets to the root of the issue - whether it be economic stress, poor family interactions or challenges, depression or other mental illness, or poor medical management of pain. I am optimistic that the American people will speak out and share their personal experiences with a direct primary care practice. Soon, the current momentum that is already motivating public and private insurance companies offering "total health " plans that has a direct care flavor or large health systems offering more ways for patients to connect with them, will lead to national support for direct care. The challenge will be for physicians to prevent corporate greed getting in the way of our patient care. To a healthier America, Dr. Ahmed  Many of you might have read the book Toyota Kata, or heard of lean management. Furthermore, many may have heard about lean health care. As the principles of lean management take over organizations across many industries, we find that the most successful organizations are those who achieve integration and implementation of these principles. But, it is not these principles alone that make an organization successful. It is the organizational culture of commitment, leadership development, empowerment, and employee investment that makes the difference.
Health care has become an industry that is one giant green monster that is zapped from many stakeholders, like the government, private corporations, pharmaceutical companies, and insurance companies, all trying to get this monster under their control. But who is really out there protecting the people? As I mature as a physician in this circus, also known as United States health care system, I am starting to realize a few things. When I was a medical director at a large health system, I saw how decisions in health care are largely led by thinking of margins before patient care. My department was not a revenue generator compared to others, but a cost savings one. But, as I continued to grow my team and expand our services, I realized that no matter how hard I tried the decisions I would make were always under the scrutiny of corporate leadership. How is this different than the practice of medicine? The decisions that physicians make "out in the field" - in clinics, hospitals, etc - are largely guided by insurance companies, government insurance, hospital policies, and pharmaceutical companies. We often hear, "that costs too much" or "my insurance does not cover that" or "they are not in my network" or when a hospital finds out a patient is not in network, the move to a different hospital happens at lightening speed! Kata, in Japanese, means a way of doing something, a pattern, or a standard form of movement. So as leaders, the challenge is to get team members implementing a routine without requiring constant input from administration. The idea is to have a routine that nurtures continuous improvement and adaptation. More importantly, decisions are pushed to those who are closest to the issue. So, when Toyota stops the line when a part is not put in correctly, the lights go off, the line stops, managers come over to help repair the part, others assist as needed, and the line resumes once corrections are made. This process is more efficient, has a team approach, allows everyone to adapt and improve the process immediately by correcting a routine to make it more efficient. Health care today, uses cost benefit analysis (CBA) to the max! The problem is that the budget is a dependent variable, not independent. Instead of CBA, health care providers and leaders must think in terms of target conditions to move towards their vision. More importantly, not only do organizational leaders must think this way, but physicians must practice this with their patients; thus, developing their patients as leaders of their health care! Here is an example of how this works, especially in primary care. If I have a overweight type 2 diabetic, my first visit might be discussing the importance of blood sugar control, diet, and how their current medications will help them prevent further organ damage. 1st step: Understand the current situation. What is their current blood sugar control and where do they want to be in terms of their diabetes control? What does the future look like? What is their overall prognosis today if their current situation does not change? This visit is truly about goal setting. As Charles Duhigg says in Smarter, Faster, Better, goals should be SMART (Specific, Measurable, Achievable, Realistic, Timeline). 2nd Step: Set SMART goals or target conditions to achieve the vision of - coming off insulin, achieving BMI less than 25, having an A1c< 6.5%, etc. Put a timeline together. Discuss potential barriers with possible solutions the patient can use when they might come across these barriers. 3rd Step: Meet frequently. I recommend every 1-2 weeks the first month. Reflect on barriers, solutions, and give feedback of how to improve to stay on tract to achieve the goal set for that month. This is the value of direct primary care, instead of the insurance model. 4th Step: Provide ongoing support and always keep focus of the patients vision. When the vision is realized, celebrate! Get feedback from the patient and provide them with your feedback so that they can lead others. In my young career, I have held a few leadership positions and have been mentored by great leaders. My Master's program was fantastic and had created a good foundation to build my experiences. All my experiences and positions in health care form my current vision for my fellow Americans: Patient leaders who then lead others in achieving their quality of life. Imagine a United States health care system that truly implemented Kata principles and SMART goals. Naturally, in this type of system, primary care becomes the most crucial aspect. It is the place where patient empowerment begins and grows. Patients as leaders of their health care must be the mindset of future health care entrepreneurs. In my company, this is how we achieve success - develop everyone around us as leaders. Whether it be patients, partners, or staff, our focus is to develop leaders. Empowered health care consumers should not be just a term we throw around. It is time we implement this belief and it is the missing ingredient our health care needs. Otherwise, we remain broken. To better health for all, Dr. Ahmed We are currently 9 months into the practice since my clinic opened and more than 12 months since I started doing house calls to spread the word about a new way of providing primary care. In the last 5 years, we have seen a shift in healthcare policy. Expanding coverage we all know does not immediately mean accessible and affordable care. In addition, we see people waving their Medicaid/Medicare or private insurance cards in the air saying, "we are insured so come see us" but there are less physicians to take care of them. More and more physicians as well as large health systems are not participating with Medicaid/Medicare or some private insurance carriers. So, before you start to feel comfortable having that plastic card in your pocket, you should spend the time to figure out exactly what you actually bought and which physicians participate with your plastic card.
 Did you know that each time you visit an ER, urgent care, or get admitted to the hospital your risk of developing anemia increases?
increased hospital stay = anemia = decrease longevity So stop running to these places to get accessible care. Primary care prevents this nonsense. Relationships matter! Build one today. Click HERE to learn more...again, beware as it is very detailed. I am pretty nerdy.  Employer wellness programs have become more popular in the last several years. Its popularity for implementation has its roots in the ever increasing concerns of rising prevalence of obesity, diabetes, heart disease, and many other chronic illnesses. In fact, based on recent surveys, almost 80% of companies offer some type of a wellness program.
Vendors for these wellness programs have enjoyed their growth in the last several years to a point where it has become a $6 billion industry. So, it is only fair to ask the question: Are employers getting a significant rate of return on their investment? The rationale for having a wellness program in the workplace is to create a organizational culture of wellness, improve the health of its employees, decrease turnover, increase productivity, reduce health care costs, and on a larger scale - improve the health of our nation. Nearly half of Americans get their health benefits from their employer and we all spend a majority of our time in the workplace. Thus, these goals and rationale make sense. But, has this $6 billion industry delivered on its promise? On average, employers spend about $693 per worker and larger companies who have 20,000 workers or more spend nearly $878 per worker. A large survey found that although some biometric markers like BMI, smoking cessation, and exercise had improved, these changes were not large enough to reduce health care costs nor provide the employer with a substantial ROI. In addition, one of the major challenges in offering a wellness program is employee engagement (industry talk for employee participation). Surveys have shown that even after a wellness program is implemented, employee engagement is low. Studies have shown that the lost productivity from employee disengagement costs between $450 billion and $550 billion annually in the United States. For each employee, disengagement can cost the employer $5,000 to $7,000 per year in lost productivity. What if a physician led an employee health benefit plan where it included resources like fitness trainers, physical therapists, nutritionist, chiropractor, acupuncture, supplements for healthy eating and weight loss, financial advisors, lawyers for estate planning, massage therapists, counselors, medical specialists, and educators? What if the physician also had partners in imaging, laboratory, pathology, had wholesale medications in their office, did not charge for any office visits or in clinic procedures like EKG, joint injections, suturing, skin biopsies, wound care, breathing treatments, or spirometry? What if each employee as part of this physician led wellness plan had 24/7 access to their physician, even during holidays? Certainly a relationship between the employee and the physician is inevitable. So is there value in this relationship where the physician understands the stresses, aspirations, goals, as well as medical condition of the employee? Finally, what if the cost is only $600 per employee that is fixed annually with no other out of pocket expenses for the employer? While the employee enjoys significantly discounted medications, imaging, laboratory, and other services. The answer to all these questions is not an ideal nor is it impossible to implement. I do it already with companies right here in Kansas City. Many physicians across the country who share my vision and mission have also aligned their practice with other companies of various sizes. In a study that reviewed insurance claims data from 2013 to 2014 showed that the employees who belonged to the Direct Primary Care model compared to those who did not saved $679,000 per 1000 employees. In addition, there were close to 20% less claims from the DPC group. Isn't it time to be innovative and offer a more comprehensive program to your employees? My practice is NOT insurance. So to qualify for the ACA mandate, employers must have a high deductible plan or a self insured plan that can be paired with our practice to give the most value to your employees. Healthcare is changing. Costs are rising and the physician supply is decreasing. Employers can play an important role in changing this landscape with one decision: partner with a direct primary care practice. Our mission is to recruit more primary care physicians, retain more physicians in private practice to facilitate patient focused care, and bring back continuity and relationship medicine. We do this simply because the health of our nation depends upon it. Please contact us today if you would like to learn more about our primary care practice and how we can partner together to truly establish wellness in the workplace. To your health - Dr. Ahmed  Recently, there has been much discussion regarding concussion and sudden cardiac death (SCD) in young athletes. Although this is rare in children and adolescents, they are so devastating when it happens. There has been a growing effort in finding evidence-based strategies that will prevent this in a cost-effective manner.
How common is this? The incidence for SCD ranges 0.5 to 20 per 100,000 persons-years. Interestingly, when we compare studies from 1980s to 2009 show a rise in survival, which is attributed to improvements in community-based EMS and changes in resuscitation protocols. What is the cause?
Interestingly: 2 years old and younger - cause of death congenital heart disease (84%) 3-13 years old - No dominant cause - congenital (21%), hypertrophic cardiomyopathy (18%), long QT Syndrome (14%) 14-24 years old - No dominant cause - Primary arrhythmia (23%), congenital (23%), and dilated hypertrophic cardiomyopathy (14%) 25-35 years old - Coronary artery disease When should I be concerned?
What is the role for screening? The American Heart Association (AHA) and the American Academy of Pediatrics (AAP) recommend that the most cost-effective initial screening for children and adolescents for cardiac disease is a detailed history and physical examination - ALONE. That is right, no need for unnecessary expensive testing no matter how some of these organizations market their services. There NO evidence that a ECG or any other cardiovascular screening program would reduce the incidence of SCD in the United States. Even for young athletes, there is NO evidence for routine use of ECG, echocardiography, or exercise stress testing. However, athletes older than 35 years old, some experts recommend ECG. If the athlete who is 35 years and older has moderate-to-high risk of coronary heart disease, then some experts would recommend exercise stress testing. Bottom line: Be careful out there as consumers are inundated with advertisements for services that can prevent cardiac disease. The truth is that unnecessary testing not only is costly, but also leads to false-positives that lead to further unnecessary testing. As with every health care topic - have a GOOD PRIMARY CARE DOCTOR to discuss issues like this and build a relationship with them so that you protect yourself from unnecessary testing that can be costly or lead to further unnecessary procedures that might expose you to harmful agents like radiation. To your health my friends, - Dr. Ahmed
Unfortunately, we give our cars, clothes, beauty/spa treatments, homes, or entertainment desires more attention than our own health. The realization of this neglect only becomes known when we become ill or injure ourselves. Therefore, just like anything else, there is tremendous value in prevention and education. One thing I hear a lot is, "I am very healthy and never see a doctor." Is that a good thing? Should we see a doctor only when we are sick and vulnerable? What about seeing the doctor to discuss life's stress, maybe you are traveling and need to learn about important vaccines, learn about any public health concerns, prevent future illness? How about losing weight? Do you really need that supplement and if so is it safe? Isn't it more costly to go to an urgent care for every minor health issue than going to a doctor who knows you and can see you that day or next day? Finally, do you really need a specialist following your chronic condition? We have new testing modalities that enable us to prevent heart attack or stroke in those who do not have the traditional risk factors, like smoking, high blood pressure, diabetes, or high cholesterol. Here is a quick chart on how our patients save if you just look at the numbers. These numbers make the following assumptions: *Single without any dependents *Male *Minimum use of health care (healthcare.gov estimates) *Cheapest plans are selected for this comparison *Average income of $75,000 *No primary care visit costs as some insurances charge $25-50 for each visit *No specialist vist costs So, if you are a couple, go to a primary care doctor currently or urgent care for your needs, have dependents, you are female, or make more money, the cost is significantly more. Remember 2016 Annual HSA Limits per IRS: Self-only coverage = $3,350 Family coverage = $6,750 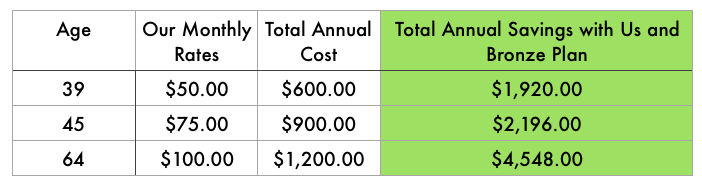 What about Medicare you ask? Well, Medicare patients not only save money, but have a physician who can be a true quarterback for your health care. Coordinating with specialists, home care services, preventing falls, making house calls or assisted living/independent living visits are a tremendous value.  This probably goes without saying, but these numbers are estimates. There are so many factors that can affect your final costs. Certainly, if you end up needing surgery or need medications, then the cost will be higher. This is simply illustrated to give you a general idea at the most basic level.
I hope this blog really clears the air a little in how insurance works with our practice. Remember, at Health Suite, you can pick LiveActive Primary Care as your primary care service or KC Family Doc. Check us out or meet us for a free consultation today! To your health, - Dr. Ahmed |
Author"He who studies medicine without books sails an uncharted sea, but he who studies medicine without patients does not go to sea at all." Archives
March 2023
Categories
All
|

 RSS Feed
RSS Feed
We are passionate about practicing medicine
|
|
CLINIC HOURS
MONDAY 9am-5pm TUESDAY 9am -5pm WEDNESDAY 9am-5pm THURSDAY 9am-5pm FRIDAY 9am-12pm Closed 12pm-1pm daily for lunch SAT&SUN CLOSED |
2024 Holidays - CLINIC CLOSED
New Year's - January 1st Memorial Day - May 27 Independence Day - July 4 & 5 Labor Day - September 2 Thanksgiving - Nov 27, 28 & 29 Christmas - December 24, 25 & 26 |
Contact Us
Tel: (913) 549-3884
Fax: (913) 273-3343
Email: [email protected]
6650 West 110th Street
Suite 220 A
Overland Park, KS 66211
Fax: (913) 273-3343
Email: [email protected]
6650 West 110th Street
Suite 220 A
Overland Park, KS 66211