|
Tis the season for the most popular sport in America, FOOTBALL! But, what is astonishing is that it is not just football where concussions occur. Sports like soccer, wrestling, basketball, ice hockey, lacrosse, volleyball, gymnastics, cheerleading, baseball/softball, and of course skiing and snow boarding. What is even more interesting is that girls report concussions more than males. Part of this might be the "macho" effect, but there is more to this than under reporting from males. It also tells us that there is more to concussions than the fact that athletes are getting bigger, stronger, and faster. Check out the study published in Clinical Sports Medicine 2011, January issue, volume 1, pages 1-17. Here is the link if you have access to this article CLICK HERE. It is also no surprise to anyone that athletic participation across genders has increased when we compare 1982-1983 to 2007-2008. But, it will blow your mind at how drastic this increase has been. Those of us who follow athletics know about the growing participation, competition, and support of high school athletics. High school athletes are also getting bigger, stronger, and faster with aspirations for professional athletics. Therefore, it is not surprising when researchers and doctors see a rise in concussions and other serious injuries in high school athletes. Understand the terminology: Concussion is a mild Traumatic Brain Injury (TBI). It is a trauma-induced alteration in mental status that may or may not involve loss of consciousness. TBI happens with head injury due to contact with acceleration/deceleration forces. Check this out:
1. Seek medical attention if either the parent or athlete notice these signs or symptoms: 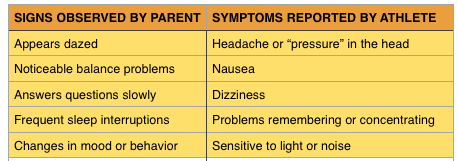 2. Treatment?
Rest from physical and mental activities. This means that television, computers, and music should be limited. That is right, NO VIDEO GAMES! These activities might make symptoms worse. Eating well balanced meals with adequate hydration are key to recovery. 3. Prevention? Play by the rules and practice good form when it comes to tackling, wrestling, etc. Identify if there are any trouble spots on the field that may increase risk for an abnormal fall. Make sure you are using the right sports equipment. Bottom line: practice good technique and focus on strengthening and conditioning. This is most important. Too many athletes focus on getting "big" or "ripped". But a good looking physique does not guarantee prevention of injury. Workout with purpose and intention. Think about the muscles your are working out. Know your anatomy. This is what makes working out fun. Take your time and take your workouts and nutrition seriously. Surround yourself with people who care about your health instead of pushing products. Being in private practice and becoming involved in my community, I meet a lot of people and small businesses. I must say, there are products out there, exercises, diets, and ideas that are just NOT SAFE. Please consult with your doctor before doing or taking anything. 4. Never ignore a head injury. When in doubt, sit the athlete out.
0 Comments
Have you ever wondered how this prescription drug abuse epidemic spiraled out of control? How did we let this happen? Who are the major stackholders? These powerful drugs were developed with a real noble purpose, but soon cycled out of control. Was it our own doing? Similar to cigarette companies, pharmaceutical executives have become significantly rich at the expense of bringing incredible harm to all of us. This is our terrible reality across all industries - greed always results in harming everyone involved. Physicians have been screaming about the dangers of these medications, but lawmakers continued to ignore them Why do we do this? Ignore the scientific community for the mighty dollar. Whether it be the approaching epidemic, rise of harmful medications or technologies, or gun control - the concern for financial profits always win. The commercial manufacturer of morphine started out in Germany in 1827. In fact, morphine was the painkiller of choice during the American Civil War. Interestingly, the doctor who invented Coca Cola formula had developed a morphine addiction during the Civil War and in their attempts to solve this issue, cocaine was sought. The new drink had cocaine mixed into it and sold to a pharmacy in Atlanta. During that time, this was perfectly legal. Heroin was created by Bayer Company in Germany in 1898. It's sole purpose was to be a remedy to the morphine addiction. Legislation, like The Pure Food and Drug Act of 1906 and Harrison Narcotic Tax Act in 1914, brought these addictive substances under the control of physicians; preventing casual distribution of these products. The current problem:
 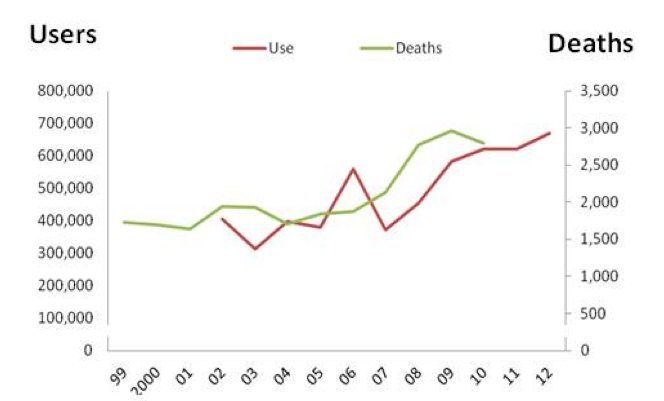 Factors that contributed to such growth:
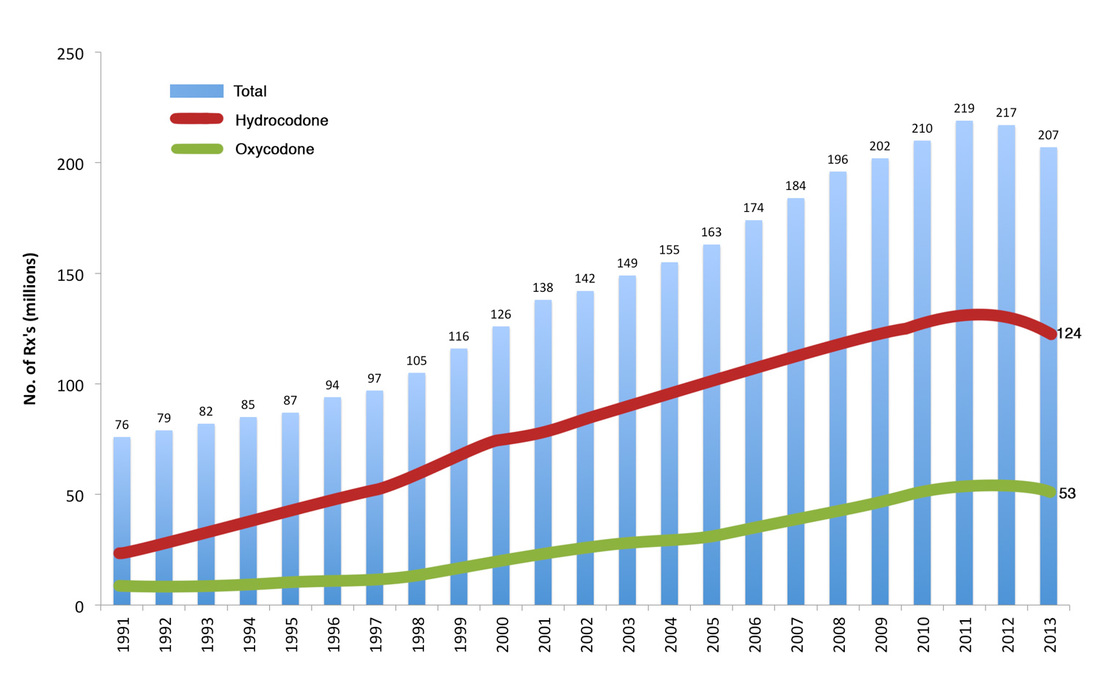
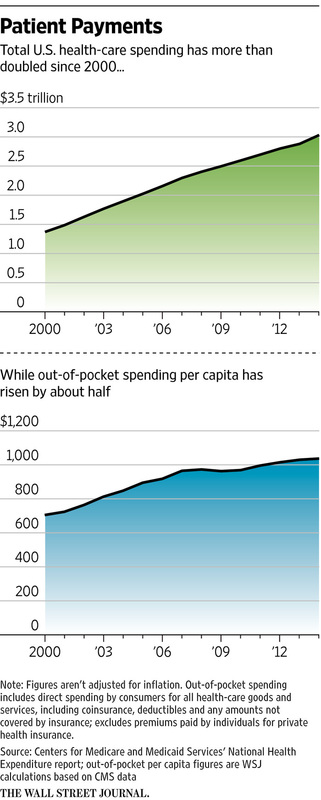
The number of prescriptions has increased from 76 million in 1991 to nearly 207 million in 2013. The United States is the biggest consumer globally. What does it mean for the pharmaceutical companies? It means more than $35 billion in sales since releasing medications like OxyContin. Annual revenues are about $3 billion for pharmaceutical companies selling prescription drugs. So, what does all this mean? Well, let's see... A medication or family of medications whose sole purpose was to help the soldiers during war starts to be sold unregulated to people around the world. Then as addiction starts to develop and people take notice, regulations are made to help control its spread, but either inadvertently or not, products like cocaine and heroin are used to "remedy" the situation. This leads to more addiction. Crap! Meanwhile, the US health system was undergoing major changes. In attempts to control costs in the 1960s-1990s major developments in public and private health plans were developed. Not too surprisingly, as the managed care organizations were attempting to control costs, US health expenditures started to rise, while reimbursement started to fall. Pharmaceutical companies started to market heavily and capitalized on a health care system that was reducing clinic visit times to an average 7-10 minutes, which led to more written prescriptions. Sound familiar? Our country has a HUGE antibiotic resistance problem where antibiotics are prescribed unnecessarily. The American public doesn't see the "super bugs" which claim many American lives where these bugs are resistant to ALL available antibiotics. Pharmaceutical companies do not invest in making more antibiotics as there is more money to be made in drugs that are taken for a long time, instead of the 5-7 days regimens that are usually prescribed for antibiotics. But, we digress. So what does the US government do to fight this epidemic? Spend more money where it doesn't matter! The President signed legislation that authorizes $181 million a year for new programs to train emergency personnel in administering drugs to reverse opiod overdoses and help communities purchase those drugs, as well as develop treatment and overdose programs. This means that pharmaceutical companies have more buyers for medications like Narcan and other products. Which leads to more profits! These treatment centers will be overwhelmed with the large demand as the public now has available "quick reversal" agents. This sends the wrong message and does NOT get to the root of the problem. Those of us who have taken care of overdose patients know that the problem does not cost so much money, development of more "reversal" agents, nor does it require capital investment to create "treatment facilities." The solution is simple: Establish a human connection involving time to talk, engage, motivate, build strong relationships, and bring people together. What does this solution look like more specifically? All physicians, including specialists, are demanding better primary care. Longer visits allow for conversation and developing a plan that may include various pain control options outside of prescription medications. The primary care setting is the place where opioid management should take place. Why not? The primary care physician is the leader of their care; the quarterback who is most likely or should be managing multiple health issues. They are the ones who spend time with the family, loved ones, might even have done a few house calls, knows what barriers exist to better health, and is the one making referrals or partnerships to bring more solutions to their delivery of care. This is what true primary care looks like. Not a place to get a referral to a pain specialist or some methadone clinic. Why do we accept such nonsense? Let the primary care doctor to what they are trained to do. The health system must support and allow this interaction to happen because this small investment will prevent huge costs in the future. Psychologists, counselors, psychiatrists, social work, and others might need to be involved. More importantly, there cannot be a delay in seeing each of these specialists and there needs to be total - 24/7 - contact between physician and patient to prevent "loss to follow up." This solution is cheaper, preserves human dignity, and most importantly it gets to the root of the issue - whether it be economic stress, poor family interactions or challenges, depression or other mental illness, or poor medical management of pain. I am optimistic that the American people will speak out and share their personal experiences with a direct primary care practice. Soon, the current momentum that is already motivating public and private insurance companies offering "total health " plans that has a direct care flavor or large health systems offering more ways for patients to connect with them, will lead to national support for direct care. The challenge will be for physicians to prevent corporate greed getting in the way of our patient care. To a healthier America, Dr. Ahmed February 1, 2015 was the day I broke free from the insurance run health care system. After several years of being a staff physician at a large health system, medical directorship, running research studies, writing articles, being a pharmaceutical consultant for 2 large companies, I realized I cannot change this system from within. Corporate greed was too great for a young physician to fight.
Each year I practiced medicine, I met another hard working American who waived his/her plastic insurance card, yet could not receive accessible or affordable primary care. I have met many other hard working Americans who couldn't get coverage regardless of the Affordable Care Act (ACA). The final story I could tolerate came when I met a 35 year old female who suffered a massive stroke and had to have her skull drilled to relieve the growing pressure from a massive brain hemorrhage. I took over her care after she had been moved from the ICU to the floor. My job was to figure out why she had the stroke, prevent the next stroke, and aggressively pursue rehab. I had triaged her as one of my last patients to see as she was reportedly stable. I knocked on the door and found a young brown haired caucasian female laying quietly in a dark room, alone. Her hair was disheveled as she had staples on one side of her scalp with part of her head shaved, allowing exposure to her staples. She looked exhausted. Unlike the other rooms, there were no flowers, no cards, no "Get Well" balloons. It was just her, a beeping IV pump, and a computer next to her bed. The guest couch and chairs sat empty in the corner of the room. The 42 inch TV was turned off. The large window provided some light as it penetrated the dark window and the window shade. Upon my entrance, she turned to look at me with sad eyes and managed to smile half way. I pulled up a chair next to her bed to listen to her story as I did with every patient. She readjusted herself, which was challenging as her entire right side was still weak. You see, she was a young 35 year old single mom who was working 3 part-time jobs, because her employers did not want to offer a full time job as that would require them to offer her health insurance under the current laws. So, she did not have insurance because of this. Her story began with a visit to an urgent care center where she was told she had high blood pressure and she was given a medication to help control her blood pressure. She didn't understand what high blood pressure would mean if it is not controlled. After taking the medication for a few days, she simply stopped taking it because to her it was all numbers and certainly didn't make her feel any "better." Besides, she was a young 35 year old and so how bad could it be? In reviewing her records, it seems she had presented to the ER with a blood pressure of 220/120. Likely, her blood pressure was the reason for her stroke and head bleed. The medication she was on for high blood pressure is $4. Needless to say, I can get this medication for my patients now for $0.87 for a month supply. As her story continued to unravel, I started to stoop lower and lower in my chair. My mind started to race with anger. How can she be so abandoned? Why did no one tell her about the importance of blood pressure? Where was the follow up visit? How is this fair? She is a contributing American citizen to our economy, yet we abandon her? To put all this in perspective, here she is as an uninsured patient with an ICU stay of 5 days, surgical drainage of blood, multiple imaging studies and labs, she couldn't move her entire right side and so will need 6-8 weeks of rehab. One of her jobs was being a waitress. There is no way she could return to this line of work. In essence, we have effectively bankrupted a young, sweet, innocent, 35 year old single mom. After she had completed her story, teary eyed, and by now I was almost laying in my chair, I straightened myself and leaned forward towards her. I said,"ma'am, I am so sorry for all this. We have failed you. I as a representative of the American health care system have failed you. For that, I am sorry." I went on to explain how important blood pressure is to control and how we can prevent another stroke. I left that room with only one thought in mind...NEVER AGAIN. Never again would I allow myself to be in that chair hearing a story like that from any of my patients. My mind was made up to offer the best primary care I can, regardless of insurance status. Many people do not hear the stories that we as physicians hear. Yes, you pay for insurance premiums, but for primary care, that insurance card likely is not getting you the best care. Think about it. Some pay $25 to over $100 in copay per visit for what? A 10-15 minute visit that feels rushed or is not comprehensive. Or be sent to a specialist, procedure, imaging study, or be prescribed pills when in reality you probably didn't need it. These decisions are made simply because there is no time to get to the root of the problem. The follow up is the most important component of primary care. Start a gameplan and then you need to follow up maybe in a week or 2 weeks. But eliminate the copays that people have to pay to make the follow up more feasible. This is where direct care makes sense and saves money. The young and healthy individuals also save money and gain value in a direct care model. Simply put, casting, medications, EKG, suturing is FREE or at a minimal cost in a direct care practice. Time and money is saved. But, think about the value. That young and healthy individual is probably going through some emotional roller coasters. What are their aspirations? How strong is their social network and who are they? Who do they spend time with and how are they dealing with any stressors they may have? Are they exercising and eating healthy? If they do exercise, then are they doing it safely? Do they practice safe sex? Where are they planning to travel? Are they overweight? Do they have family history of diabetes or heart disease that predisposes them to these conditions? These questions are so important that essentially a life can be saved by simply talking to them. These young adults are connected to their physician by a simple text or video chat under a direct care model. How neat is that? This is the value of direct care with or without health insurance. Take the time to understand what you are paying for when purchasing a health insurance plan. Our patients with Medicare and supplement insurance will say the value of access, coordination of care, and availability overwhelms the minimal monthly cost. Health insurance and direct care together make a phenomenal resource for all Americans to live well. Quality of life will be enhanced. Our health expenditures will go down. Taxes will be reduced and employers will be able to retain their talented workforce. Increase in direct care practices will solve the primary care shortage, lead to more young physicians embracing private practice to revive the practice of medicine, technology will be used to bring accessible health care into the home, and the American people will be empowered to navigate the health care system with more confidence. Together, we will achieve a healthier America. Give a direct primary care practice some consideration. Visit iwantdirectcare.com to learn where the nearest direct care practice is for you. Welcome to the new US Health Care System! Dr. Ahmed
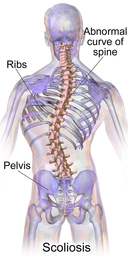
Scoliosis, as many of you know, means lateral curvature of the spine. It is a structural alteration that can progress as the person grows, leading to significant deformity. Adolescent idiopathic scoliosis (AIS) is typically defined as curvature greater than 10 degrees. Curvatures that are less than 10 degrees have no long term clinical significance.
The 3 subcategories include: - Infantile (0-3 years) - Juvenile (4-9 years) - Adolescent (>10 years) So how common is AIS? The prevalence of AIS is approximately 3% and only 10% of those adolescents require treatment. Males and females are affected equally. However, the risk for curve progression is 10 times higher in females than males. The degree of curvature is measured by Cobb angle. When considering prevalence, think about this:
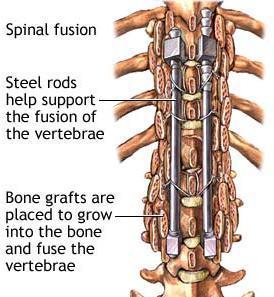
So if a family member or friend has scoliosis, first appreciate their strength and uniqueness, and then ask about their angle if they wish to share. Knowing that piece, one can greatly appreciate the prevalence of their condition. It may surprise you, but your primary care doctor can screen for scoliosis, diagnose, order the X-ray, and even start brace treatment if needed. If surgery is indicated, your primary care doctor can coordinate efficiently with an orthopedist. Point is, don't run to an orthopedist the minute you hear about scoliosis. This diagnosis, like any other diagnosis, requires a conversation. What does having scoliosis mean? Do I have to have surgery? What are the post surgical challenges I may encounter as I am recovering? Even after treatment, what should I worry about? What about pregnancy? What about sports or even contact sports? Is this genetically linked that I need to have my kids screened? What about working out - any precautions I should take? So, what does all this mean in adulthood? Regardless of getting treatment or not, there definitely are clinically significant concerns one may face as they enter adulthood. Even when the spine is corrected to midline with surgery, individuals must be cautious when weight training, aerobic activity, and may have chronic back pain. The muscles that support the spine have to adjust and may be prone to strain. Rotation is largely limited in the surgically treated spine, so one may not be able to participate in some activities. Mental health studies have yielded conflicting results based on surveys. My opinion is that this only reminds us that diagnoses are perceived differently by each one of us. I argue that your perception of your diagnosis, whatever it may be, is facilitated by your team of doctors. As physicians, we have a duty to treat illness, but also to be a coach, a friend, and most importantly a partner in any journey that requires chronic management. Positive thinking and supportive behavior has shown study after study to improve outcomes - that is the job of the physician. Be a true advocate and partner. After surgical correction, pulmonary function improves, but skeletal alignment may still have long lasting joint pains. In those patients where surgical correction is not done, the curvature can progress and cause more pain with pulmonary issues. As our bones get weaker with age, the spine may slump even more leading to alteration of your gait. Surgical correction at times requires repeat operations, scar healing, and hospitalizations can be prolonged. Thus, the sooner we can screen and treat, the better outcomes we get. Self-image might be an issue in adolescents. Wearing a brace or having visible scars after surgery may leave keloids that challenge an adolescents self image. Scoliosis is a condition that must be identified early, have a management plan, and must be included in long term management. This is not, like any other diagnosis, something that is "repaired" and forgotten. Build a relationship with your primary care physician to be at your side as you enjoy the many blessings life has given you. Nothing is impossible. We just have to make some adjustments with the challenges that are thrown our way. Please help me raise awareness about scoliosis and I hope I taught you something new about this condition that you may not have known before. To your health and our community, Dr Ahmed  Memorial Day was originally established to celebrate Civil War heroes in a single unified day, instead of separate days celebrated by the Union and Confederate states. Around the 19th century, Memorial Day expanded to celebrate all veterans who fought as American forces. As physicians, we learn from one another and are united in our thirst for knowledge to better serve humanity . War, in all its ugliness and chaos, demands innovation in science and technology. Thus, it is not surprising that modern medicine seems to have strong roots during times of war. The ancient philosophers and scientists created a foundation for physicians during the Civil War to innovate to meet the demands of its wounded soldiers, but also to create standards of care that we practice even today. Here are 5 innovations that were developed during the Civil War: 1. LIFE SAVING AMPUTATION - The old practice of saving limbs with wound cleaning using rats and maggots was replaced with cutting off infected limbs to prevent the spread of infection. In fact, Union soldiers were known for amputations, had less mortality from their procedures, and took no more than 6 minutes to perform. The technique not to cut through joints and to cut far away from the heart as possible became the standard of care. 2. THE ANESTHESIA INHALER - Stonewall Jackson's surgeon recommended the removal of his left arm after it was injured during friendly fire. When a chloroform-soaked cloth was placed over his nose, General Jackson muttered, "What an infinite blessing," before going limp. The cloth was inefficient as the liquid evaporated quickly, so Dr. Julian John Chisolm invented a 2.5 inch inhaler. Chloroform was dripped through a perforated circle on the side onto a sponge in the interior - the patient inhaled through tubes and the vapors mixed with air. This new method required less liquid; thus, allowing the physicians to treat more soldiers and using less supplies. 3. CLOSING CHEST WOUNDS - Benjamin Howard, an assistant surgeon, was told to do busy work while his superiors performed the surgeries. He started to experiment and realized that if he closed the chest with staples and linen, the lungs did not collapse as they did when the chest cavity is opened from negative pressure; thus, there was no suffocation. Survival rates quadrupled with this new technique. This technique became the standard treatment. 4. FASCIAL RECONSTRUCTION 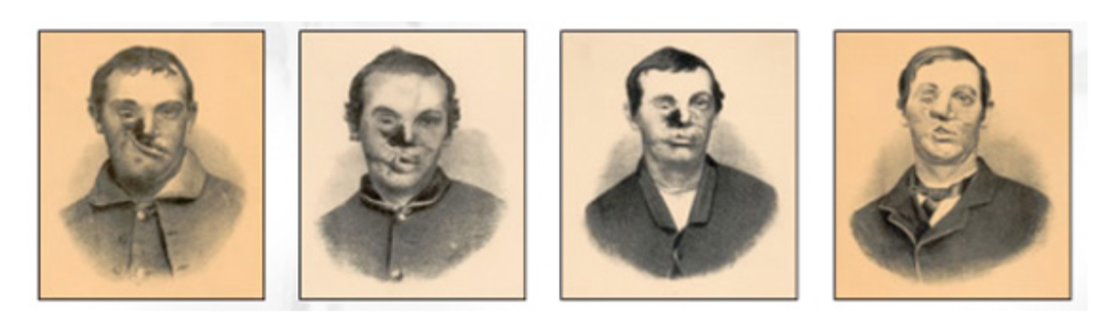 Dr. Gurdon Buck, father of modern plastic surgery, looked onto a young 20 year old private named Carleton Burgan of Maryland. This private had battled pneumonia and now the mercury pills had led to gangrene that was moving from his mouth to his eyes. His right cheekbone had to be removed and the young man was willing to try anything to stop the infection. Dr. Buck was the first to photograph his progress of his repairs and use tiny sutures to minimize scarring.
5. THE AMBULANCE-TO-ER SYSTEM - The Union went into the First Battle of Bull Run on July 21, 1861 not expecting a true battle. As approximately 1,011 Union soldiers lay wounded, the ambulances remained empty, leading to high numbers of mortality. The civilian drivers at the time were, according to some, described as "cowards" or "drunkards." Jonathon Letterman, the medical director of the Army of the Potomac, created a model of triage that we all know today. He established caravans of 50 ambulances, each with a driver and 2 stretcher bearers. He hired private wagons to carry medical supplies. The ambulances had spring suspensions and a lock box to prevent soldiers from stealing protein, bedsacks, and morphine that was reserved for the injured. Every war brings innovation and the medical community must not forget the sacrifices made by soldiers, scientists, physicians, and several other professionals who made modern day medicine what it is today. In this reflection, we must ask the question, have we been effective in preserving that fundamental drive that our predecessors had to innovate to help a large number of people without regard to creating any complex systems that may interfere in allowing the injured to access the innovation? Memorial Day should make all of us pause and reflect on the many lessons learned across all professions during our times of war. What is even more fascinating is that those lessons continue to teach us today; regardless of how advanced we think we are as a society. In loving memory of all fallen soldiers, Dr. Ahmed  Many of you might have read the book Toyota Kata, or heard of lean management. Furthermore, many may have heard about lean health care. As the principles of lean management take over organizations across many industries, we find that the most successful organizations are those who achieve integration and implementation of these principles. But, it is not these principles alone that make an organization successful. It is the organizational culture of commitment, leadership development, empowerment, and employee investment that makes the difference.
Health care has become an industry that is one giant green monster that is zapped from many stakeholders, like the government, private corporations, pharmaceutical companies, and insurance companies, all trying to get this monster under their control. But who is really out there protecting the people? As I mature as a physician in this circus, also known as United States health care system, I am starting to realize a few things. When I was a medical director at a large health system, I saw how decisions in health care are largely led by thinking of margins before patient care. My department was not a revenue generator compared to others, but a cost savings one. But, as I continued to grow my team and expand our services, I realized that no matter how hard I tried the decisions I would make were always under the scrutiny of corporate leadership. How is this different than the practice of medicine? The decisions that physicians make "out in the field" - in clinics, hospitals, etc - are largely guided by insurance companies, government insurance, hospital policies, and pharmaceutical companies. We often hear, "that costs too much" or "my insurance does not cover that" or "they are not in my network" or when a hospital finds out a patient is not in network, the move to a different hospital happens at lightening speed! Kata, in Japanese, means a way of doing something, a pattern, or a standard form of movement. So as leaders, the challenge is to get team members implementing a routine without requiring constant input from administration. The idea is to have a routine that nurtures continuous improvement and adaptation. More importantly, decisions are pushed to those who are closest to the issue. So, when Toyota stops the line when a part is not put in correctly, the lights go off, the line stops, managers come over to help repair the part, others assist as needed, and the line resumes once corrections are made. This process is more efficient, has a team approach, allows everyone to adapt and improve the process immediately by correcting a routine to make it more efficient. Health care today, uses cost benefit analysis (CBA) to the max! The problem is that the budget is a dependent variable, not independent. Instead of CBA, health care providers and leaders must think in terms of target conditions to move towards their vision. More importantly, not only do organizational leaders must think this way, but physicians must practice this with their patients; thus, developing their patients as leaders of their health care! Here is an example of how this works, especially in primary care. If I have a overweight type 2 diabetic, my first visit might be discussing the importance of blood sugar control, diet, and how their current medications will help them prevent further organ damage. 1st step: Understand the current situation. What is their current blood sugar control and where do they want to be in terms of their diabetes control? What does the future look like? What is their overall prognosis today if their current situation does not change? This visit is truly about goal setting. As Charles Duhigg says in Smarter, Faster, Better, goals should be SMART (Specific, Measurable, Achievable, Realistic, Timeline). 2nd Step: Set SMART goals or target conditions to achieve the vision of - coming off insulin, achieving BMI less than 25, having an A1c< 6.5%, etc. Put a timeline together. Discuss potential barriers with possible solutions the patient can use when they might come across these barriers. 3rd Step: Meet frequently. I recommend every 1-2 weeks the first month. Reflect on barriers, solutions, and give feedback of how to improve to stay on tract to achieve the goal set for that month. This is the value of direct primary care, instead of the insurance model. 4th Step: Provide ongoing support and always keep focus of the patients vision. When the vision is realized, celebrate! Get feedback from the patient and provide them with your feedback so that they can lead others. In my young career, I have held a few leadership positions and have been mentored by great leaders. My Master's program was fantastic and had created a good foundation to build my experiences. All my experiences and positions in health care form my current vision for my fellow Americans: Patient leaders who then lead others in achieving their quality of life. Imagine a United States health care system that truly implemented Kata principles and SMART goals. Naturally, in this type of system, primary care becomes the most crucial aspect. It is the place where patient empowerment begins and grows. Patients as leaders of their health care must be the mindset of future health care entrepreneurs. In my company, this is how we achieve success - develop everyone around us as leaders. Whether it be patients, partners, or staff, our focus is to develop leaders. Empowered health care consumers should not be just a term we throw around. It is time we implement this belief and it is the missing ingredient our health care needs. Otherwise, we remain broken. To better health for all, Dr. Ahmed Climate change, according to the EPA, means that the Earth is warming. In fact, the average temperature has risen 1.5 degrees Fahrenheit over the past century. It is expected to rise another 0.5 to 8.6 degrees Fahrenheit over the next hundred years. Why should we care and as a physician, what does this mean to our health? This is an important topic. So important, in fact, that the American College of Physicians (ACP) has written a position paper on this matter. The rising temperatures have led to changes in weather and climate. This means more floods, droughts, intense rain, and more frequent and severe heat waves. Oceans are heating up and becoming more acidic and with glaciers melting, sea levels are rising. Many bacteria, insects, and other disease causing organisms thrive in these environments. You see, insects are effective carriers and vehicles for spreading disease to large populations. The Zika virus, Lyme disease, West Nile Virus, Ehrlichiosis, and the list goes on. In addition, water is at risk of becoming contaminated and the air is becoming more polluted and full of allergens, which lead to significant health hazards from infectious disease to cardiovascular and respiratory illnesses. The health effects are already being felt by all of us, especially physicians. The number of emphysema exacerbations, sinusitis, allergies, asthma flares, and respiratory failure from these pathologies is increasing in frequency and severity. The number of strokes and heart attacks in young and healthy individuals are increasing - in fact, I tweeted a NY Times article a few months ago that raised this concern. I was in the doctors lounge last weekend and talking with a critical care friend of mine. As we sat there talking about our day, I asked him "how has the flu season been?" To this he responded, "we had worse years, but still lost a few." To us, the stories of healthy 18 year olds going on ECMO - life saving bypass machines- are not extraordinary. Unfortunately, it is all too common. In our experience, we have seen and heard of many young healthy folks pass away from things like the flu or an asthma flare triggered by allergies. Cases of infectious disease from contaminated water or food poisoning are also common. Ultimately, cases that come from contaminated food and water that should have been "ancient" are present and claim many lives today. It is hard to convince the general public about the importance of climate change and it's effect on all of us. Thus, we write position papers, use TV, radio, and journals to get the word out. But like any other health issue, as much as physicians long for conversations like this to take place before any crisis happens, it almost always ends up being at the bedside surrounded by concerned family members. The issue of climate change transcends countries, race, nationalities, or gender. This is a human issue. It's a international issue that must be taken seriously by each of us. Like many health challenges and pathologies, there are solutions and steps we can take today to prevent the development of global disease and fatalities. Please read the ACP position paper published yesterday and also visit www.epa.gov to learn more about how you can help.
We are currently 9 months into the practice since my clinic opened and more than 12 months since I started doing house calls to spread the word about a new way of providing primary care. In the last 5 years, we have seen a shift in healthcare policy. Expanding coverage we all know does not immediately mean accessible and affordable care. In addition, we see people waving their Medicaid/Medicare or private insurance cards in the air saying, "we are insured so come see us" but there are less physicians to take care of them. More and more physicians as well as large health systems are not participating with Medicaid/Medicare or some private insurance carriers. So, before you start to feel comfortable having that plastic card in your pocket, you should spend the time to figure out exactly what you actually bought and which physicians participate with your plastic card.
 Did you know that each time you visit an ER, urgent care, or get admitted to the hospital your risk of developing anemia increases?
increased hospital stay = anemia = decrease longevity So stop running to these places to get accessible care. Primary care prevents this nonsense. Relationships matter! Build one today. Click HERE to learn more...again, beware as it is very detailed. I am pretty nerdy.  WARNING: This blog is very geeked out, so it is NOT for the casual reader. The health and fitness industry has grown to become a multi-billion dollar industry. A large part of this growth has been through selling supplements to the “busy” consumer who just does not have time to eat healthy. Or, these products target the average American who has the aspirations to have the body like their favorite athlete. This has led to an explosion of various products confusing the consumer as to what is really necessary to take. The goals of this post are: 1. Understand basic human physiology of muscle contraction and all the micronutrients that are involved 2. Educate regarding these micronutrients and how supplements aim to help, assist, or replace them 3. Learn about various supplements, including pre-workout drinks, branched chain amino acids (BCAAs), creatine, B vitamins, and much more! 4. Touch on the topic of probiotics and fiber. What's my colon got to do with all this? 5. Touch on "detox" programs, juicing, and fasting. Which is better and do I really need to do this? Throughout this discussion, there is one proven fact that cannot be dismissed: all the nutrients your body needs already exist in your environment. To eat and live healthy, all we have to do is be willing to learn, make healthy eating a priority, and surround ourselves with people who will support eating healthy. Easy as that. To learn more, check out Dr. Sommer White, a board certified physician who is a great resource for you to learn about how food can heal and facilitate healthy living. http://www.sommerwhitemd.com Also consider reviewing my previous blog about the 7 essentials to live healthy. Basic physiology of energy We all need energy to do anything. This is a law of physics where energy that is kinetic (motion) is dependent on the weight of the object and its speed. So the faster it moves and heavier it is, the more kinetic energy it develops. Energy = weight (kg) x velocity (m/s2) In food, we measure energy in calories. Our sources of energy come from proteins and carbohydrates. 1 calorie = 4.1868 Joules (measurement of energy in an object)  There is international debate as to how much calories we should consume. But here is a general recommendation: Men = 2500 daily calories Women = 2000 daily calories Those who are sedentary, certainly these requirements will suffice. But, what about those who are active. Meaning, those who are working out 150 minutes per week or more? Active individuals have a higher demand for micronutrients and calories, especially if they want to maintain their weight and/or muscle mass.  This means, that the more you exercise, the more you expend energy, then the more you need to invest in the recovery phase. The recovery phase means:
It is the recovery phase where you build muscle, not when you are working out in the gym. Remember, before a single muscle fiber moves, it needs to get a signal from the nervous system. This is called an action potential. This process involves sodium and potassium channels. This is why micronutrients are so important! Basic muscle physiology Our muscles are important structures as they not only give us strength, make us look “buff”, but also strengthen joints and improve our balance as we age. To learn what an action potential is watch this video. I love this guy because this is what I probably would be doing if I didn't become a doctor. Now that you understand the basic muscle physiology and realize all the micronutrients that are involved in the contraction, the following sections will make more sense. What about these pre-workout drinks? There are various drinks on the market. At the gym, I see few people still use Monster energy drinks and the like. More commonly, I see 5-Hour energy. The main component in many of these drinks is caffeine. 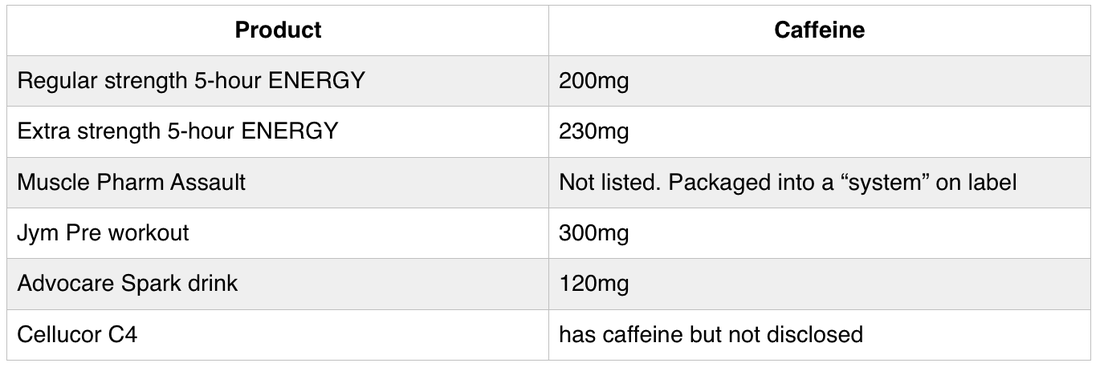 *Depending on the brew, an 8oz serving of coffee contains anywhere from 60-120mg of caffeine. Tea averages about 20-90mg per 8oz cup. Soft drinks average 20-40mg per can. How much caffeine is too much? According to the Mayo Clinic, up to 400mg of caffeine a day is safe in healthy adults. However, in adolescents and children, they should limit to no more than 100mg of caffeine per day. So, taking a pre-workout drink will get an adult close to or meet that maximum daily requirement. Remember, these recommendations are for healthy adults. If you have heart disease, high blood pressure, anxiety, high cholesterol, arrythmias, and many other health conditions, then these recommendations DO NOT apply to you. Here is where having a good primary care doctor can help. Have a good conversation about your workout goals and work together to reach those goals in a healthy way. If your current primary care doctor is not comfortable with this conversation or doesn't even workout…well, then give Dr. Ahmed a call! Many energy drinks and pre-workout drinks are packed with B vitamins. Ever wonder why? Check this out: 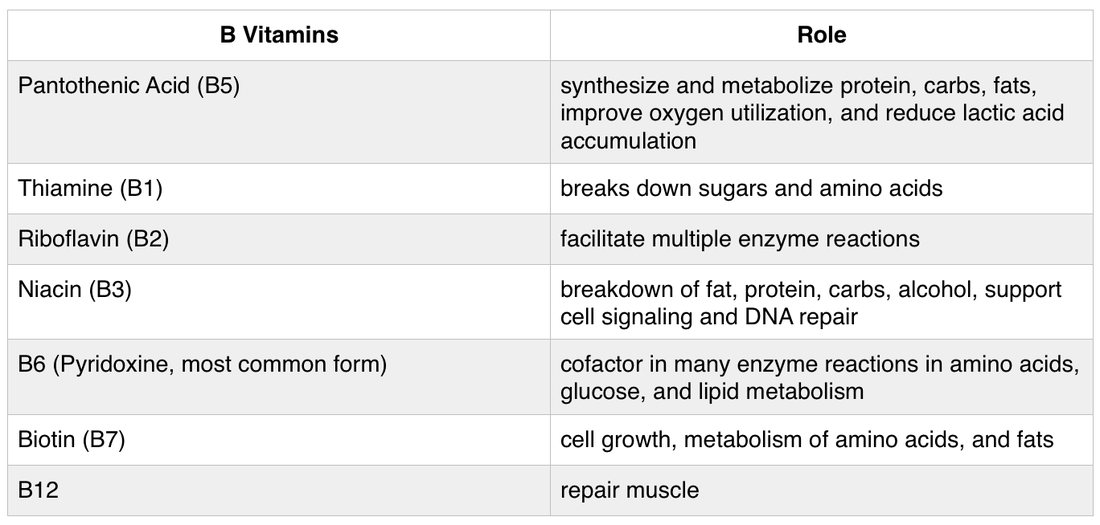 What about whey protein and branched chain amino acids (BCAAs)? Or, creatine and glutamine so I can look like those fitness models? Because clearly, if I take all those, I will look like them right? Um, no you will not look like those fitness models just by taking these supplements. It takes a good balanced diet and exercise. More specifically, 80% - 90% is diet and the rest is exercise. You read that right: diet is more important than your exercise regimen. How about juicing, fasting, and all these “detox” programs? Majority of these programs are sketchy and very dangerous. Regardless of which program you are following, you need to be followed by a physician. This idea of “detox” should be an ongoing program where you eat foods that help clear any toxins by allowing normal bowel movements, increasing the efficiency of our cellular enzymes and reactions to digest all the toxins we are exposed to in our foods, water, air, etc. Check out www.sommerwhitemd.com. Watch her videos and her explanation of detoxification approach through food. We had her at our clinic and support what she offers. Short intervals of fasting are healthy, but must be monitored by a physician. Juicing has similar advantages for detoxification with elimination of inflammatory markers and provide antioxidants. Again, this should not be a one time thing and must be monitored by a physician. The bottom line is, get a doctor to monitor and assure that whatever you choose to do, follow it up with eating a healthy balanced diet and exercising daily. At the end of the day, diet and exercise is what is going to give you the benefits. If a fast or a juice helps you transition or get you to diet and exercise, then do it I guess. Here is a breakdown of the most popular ingredients the average athlete is curious about? 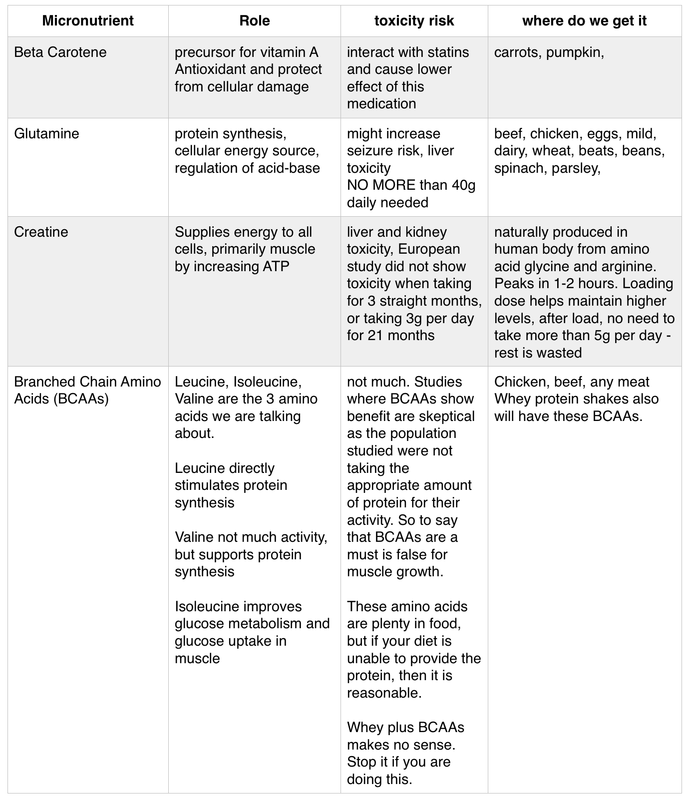 How much protein do I really need? The average person needs about 1g/kg of protein per day. Those who are not as active can probably be ok eating a little less than that. However, if you are trying to add muscle mass, then the usual recommendation is 1.5g/kg. Remember, muscle building happens at night when you are sleeping or when you are resting, not at the gym. Balance this with about 30g of fiber to prevent constipation and certainly anyone with kidney disease, high blood pressure, or the medical conditions must be monitored by a physician. To give you some idea of how much protein some common foods have:
So, the point is, before you run to the store to get containers of whey protein and bottles of BCAAs, think about how much protein you already consume and if there is a deficit, THEN consider possibly supplement. Remember, many if not all supplement products are NOT FDA approved. This means, these supplements are not benign or harm free. We just do not know the long term effects of some of these supplements. That is why I recommend use supplements to help you fill in gaps and hopefully you can replace those supplements with actual food. Long term supplements are not a good idea since we do not have the data to support their absolute need for the average human being. Professionals athletes are a different category in this discussion. Probiotics and colon health There has been more enthusiasm about probiotics recently without the support of much scientific evidence. All the trials that are done on probiotics are inconsistent with methodology or are small studies. The intestinal tract is a host to any bacteria and any change in these colonies can affect your health. In a sense our intestine has its own ecosystem with bacteria regulating certain toxin elimination and protecting the intestine from inflammation and other processes that can damage its lining. By definition, probiotics are microorganisms that have beneficial properties for the human being. Many of the bacteria in these tablets are available in foods, such as non-pasteurized yogurt and milk. Some of the benefits include suppression of growth or epithelial binding/invasion by pathogenic bacteria, improvement of intestinal barrier function, modulation of the immune system, and modulation of pain perception. Reports for benefit have been seen in the following conditions: 1. infectious diarrhea 2. Clostridium deficile infection 3. preventing antibiotic associated diarrhea 4. Possible benefit with IBS *Again, the data is limited here. As you can see, there are only a few things have shown moderate evidence of benefit Fiber is a stool bulking agent that helps people stay regular. It is important to have one bowel movement per day. The bulking agent facilitates peristalsis, which is contraction of the intestinal tract to help move stool along to facilitate a bowel movement. You need to take in about 20-25g of Fiber daily. I usually recommend 30g given the poor American diet. You can get fiber in a balanced diet or supplement with any affordable over the counter powders. Colon health is important to eliminate toxins from our body. If you think about it, our body eliminates waste by sweating through our skin, urination, and stool elimination. The average American does not stay hydrated and nor do they stay regular with their fiber intake. So the body is left with only sweat as a mechanism to eliminate waste. There is something to be said as these toxins accumulate and are not released, this can lead to poor health outcomes. More evidence is needed for this statement to be completely accurate, but the basic physiology suggests this possibility. What is the bottom line on supplements?
I take supplements to help with muscle development and recovery. However, supplements are there to do just that - supplement your diet! A majority of supplements I think are unnecessary long term. If you are working out for a competition or a sport, then short intervals are reasonable. The more I learn about various vegetables that I had no idea about: daikon, miso, wakame, dried shiitake, and the benefits of brown rice, I am starting to realize how silly supplements seem. Every supplement, whether they claim to be “all natural” or not, need to be monitored by a physician who is comfortable with these products. I have tried many supplements and do so with the intent to taste what my patients or future patients are likely trying. I also read about these products, because for me, it is important to have a knowledgable discussion about these products in the right medical setting. Consumers who take these products are likely very in tune with their bodies and would appreciate a physiologic lesson as to why they should continue, adjust their dose, or maybe even stop what they are taking. So, bottom line, focus on your diet. Get a team together that will help you not only understand but hold you accountable to a good balanced diet. Food should be entertaining, enjoyed with company, and diverse to facilitate curiosity and enjoyment. The supplement industry makes billions off the human behavior of not sticking to a plan or climbing on and off the wagon. Save yourself money and put together a good team for yourself to help you take what you need and stick to a program for life. Finally, combine your healthy diet and supplements with the right exercise program. You do not need to work out 6 days a week and spend hours at the gym. After 1 hour in the gym of active working out, any more time is just increasing your risk for injury. Athletes are different in that they know how to recover in between training sessions during the day with the right nutrition to allow healing of those injured muscles. Don’t be swayed by these new years resolution gimmicks. Stick to what you know - great diet with 150 minutes of activity per week is all you need to see results. Finally, be patient and positive. Feed your soul with a good book, meditate, do yoga, and laugh. Please do no hesitate to ask any questions you may have. Better yet, if you don't have a primary care doctor, please consider joining my practice. To a great year full of happiness, health, and blessings, Dr. Ahmed |
Author"He who studies medicine without books sails an uncharted sea, but he who studies medicine without patients does not go to sea at all." Archives
March 2023
Categories
All
|
||||||
 RSS Feed
RSS Feed
We are passionate about practicing medicine
|
|
CLINIC HOURS
MONDAY 9am-5pm TUESDAY 9am -5pm WEDNESDAY 9am-5pm THURSDAY 9am-5pm FRIDAY 9am-12pm Closed 12pm-1pm daily for lunch SAT&SUN CLOSED |
2024 Holidays - CLINIC CLOSED
New Year's - January 1st Memorial Day - May 27 Independence Day - July 4 & 5 Labor Day - September 2 Thanksgiving - Nov 27, 28 & 29 Christmas - December 24, 25 & 26 |
Contact Us
Tel: (913) 549-3884
Fax: (913) 273-3343
Email: info@Liveactivepc.com
6650 West 110th Street
Suite 220 A
Overland Park, KS 66211
Fax: (913) 273-3343
Email: info@Liveactivepc.com
6650 West 110th Street
Suite 220 A
Overland Park, KS 66211